Sha Yun, Xu Rui, Shao Shihao, Yang Jinyuan, Tang Beining, Liang Qingna, Wang Zhonghui
Department of Anesthesiology, The Third Affiliated Hospital of Kunming Medical University, Yunnan Cancer Hospital, Peking University Cancer Hospital Yunnan, Kunming, China.
Department of Urology, The Second Affiliated Hospital of Kunming Medical University, Kunming, China.
J Thorac Dis. 2025 Jul 31;17(7):5371-5387. doi: 10.21037/jtd-2025-314. Epub 2025 Jul 28.
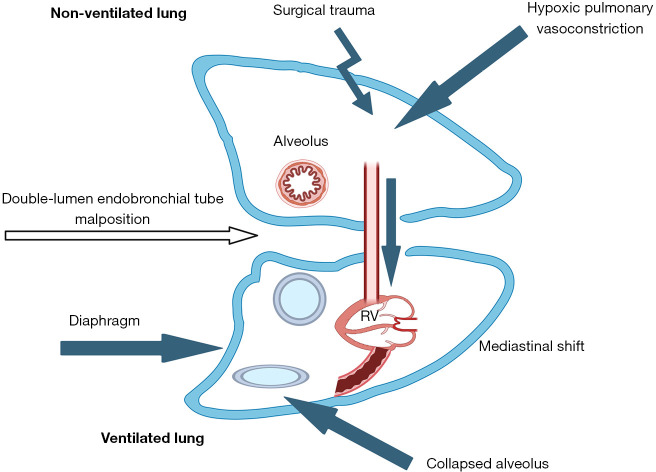
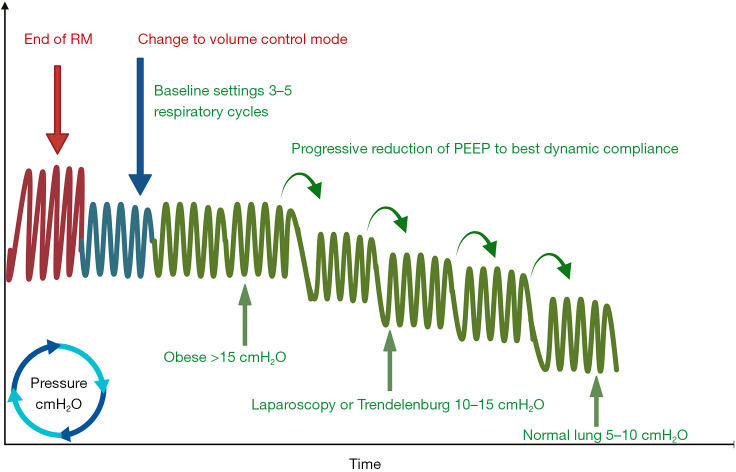
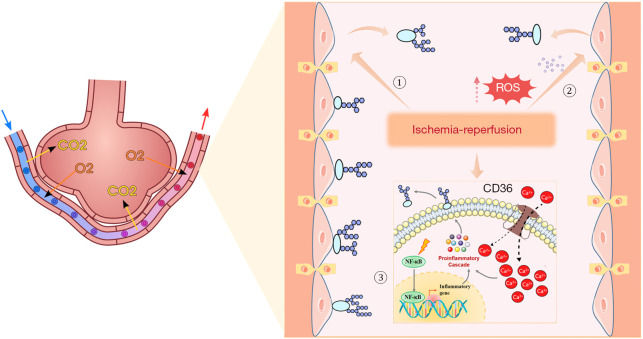
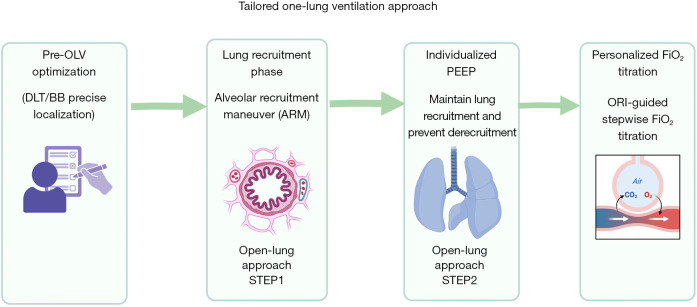
Traditional lung-protective ventilation [low tidal volume (VT) with fixed positive end-expiratory pressure (PEEP)] reduces intraoperative lung injury but exhibits limited efficacy in preventing postoperative pulmonary complications (PPCs) following thoracic surgery requiring one-lung ventilation (OLV). This review systematically examines the multifactorial mechanisms of OLV-associated lung injury, encompassing hypoxemia [device malposition, atelectasis, ventilation/perfusion (V/Q) mismatch, impaired hypoxic pulmonary vasoconstriction (HPV)], oxidative stress, ischemia-reperfusion injury (IRI) (glycocalyx degradation, mechanical stress, inflammation), and ventilator-induced trauma (volutrauma, biotrauma). To address these limitations, we propose an open-lung protective ventilation strategy integrating alveolar recruitment maneuvers (RMs) with individualized PEEP (iPEEP) titration based on optimal respiratory compliance. Furthermore, we innovatively introduce oxygen reserve index (ORI)-guided titration of fraction of inspired oxygen (FiO), enabling dynamic determination of the minimum effective FiO to mitigate hyperoxia-related toxicity. This synergistic "RM-iPEEP-FiO triad" facilitates personalized intraoperative respiratory management by stabilizing alveoli, optimizing V/Q matching, and minimizing oxidative stress, thereby significantly reducing PPCs risk compared to conventional fixed-parameter approaches. Current limitations include insufficient multicenter validation, technical dependency on advanced monitoring/ventilators, and lack of subgroup analyses for high-risk populations. Future research should prioritize multicenter randomized controlled trials to establish universal thresholds for tailored parameters. Integration of artificial intelligence (AI) for real-time respiratory mechanics analysis and multimodal imaging is essential to refine precision thresholds. Ultimately, this strategy aims to establish an evidence-based, precision perioperative ventilation framework that optimizes clinical outcomes in thoracic surgical patients by overcoming the constraints of standardized ventilation protocols.
传统的肺保护性通气(低潮气量[VT]加固定呼气末正压[PEEP])可减少术中肺损伤,但在预防需要单肺通气(OLV)的胸科手术后的肺部并发症(PPC)方面疗效有限。本综述系统地研究了OLV相关肺损伤的多因素机制,包括低氧血症(设备位置不当、肺不张、通气/灌注[V/Q]不匹配、缺氧性肺血管收缩[HPV]受损)、氧化应激、缺血再灌注损伤(IRI)(糖萼降解、机械应力、炎症)和呼吸机诱导的创伤(容积伤、生物伤)。为解决这些局限性,我们提出了一种开放肺保护性通气策略,将肺泡复张手法(RM)与基于最佳呼吸顺应性的个体化PEEP(iPEEP)滴定相结合。此外,我们创新性地引入了氧储备指数(ORI)指导的吸入氧分数(FiO)滴定,能够动态确定最小有效FiO以减轻高氧相关毒性。这种协同的“RM-iPEEP-FiO三联征”通过稳定肺泡、优化V/Q匹配和最小化氧化应激,促进个性化的术中呼吸管理,从而与传统固定参数方法相比显著降低PPC风险。当前的局限性包括多中心验证不足、对先进监测/呼吸机的技术依赖以及缺乏对高危人群的亚组分析。未来的研究应优先进行多中心随机对照试验,以建立定制参数的通用阈值。整合人工智能(AI)进行实时呼吸力学分析和多模态成像对于完善精确阈值至关重要。最终,该策略旨在建立一个基于证据的、精确的围手术期通气框架,通过克服标准化通气方案的限制优化胸科手术患者的临床结局。