Luo Lingyun, Luo Xuelian, He Zhen
Department of Cardiology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan 430030, Hubei, China.
Hubei Provincial Engineering Research Center of Vascular Interventional Therapy, Wuhan 430030, Hubei, China.
Am Heart J Plus. 2025 Aug 4;57:100587. doi: 10.1016/j.ahjo.2025.100587. eCollection 2025 Sep.
Serum uric acid (SUA) and renal status are associated with the Cardiovascular-Kidney-Metabolic (CKM) syndrome. However, the causal association among them along with drug therapy need to be explored.
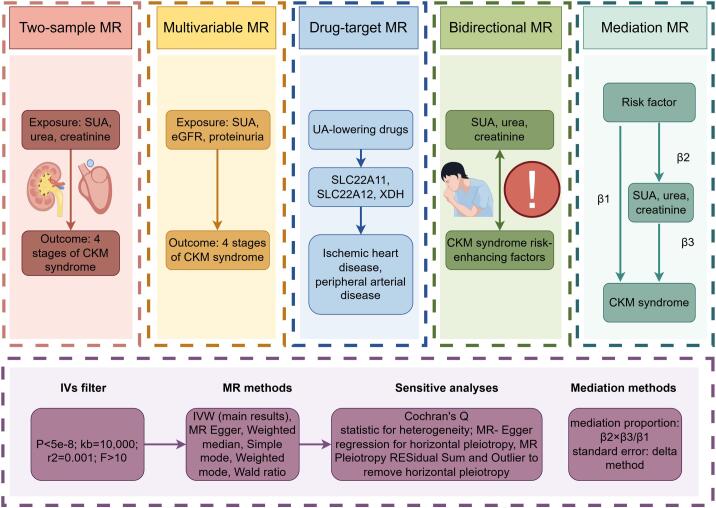
We employed univariable, multivariate, mediation and drug-target mendelian randomization. Inverse variance weighting was the primary result, with extensive sensitivity analyses conducted to ensure robustness and reliability.
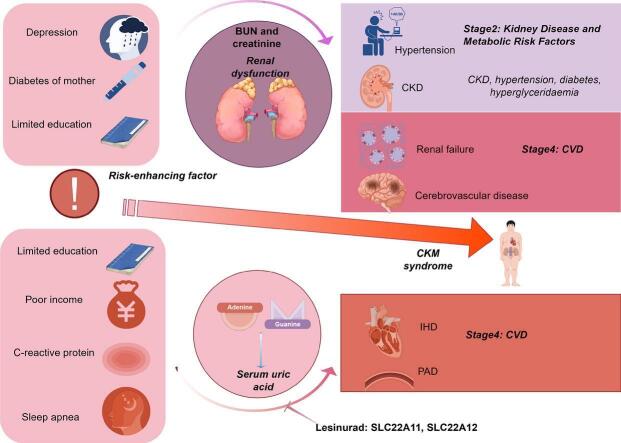
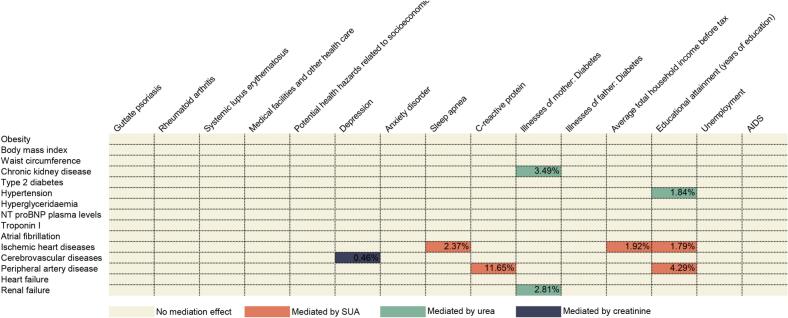
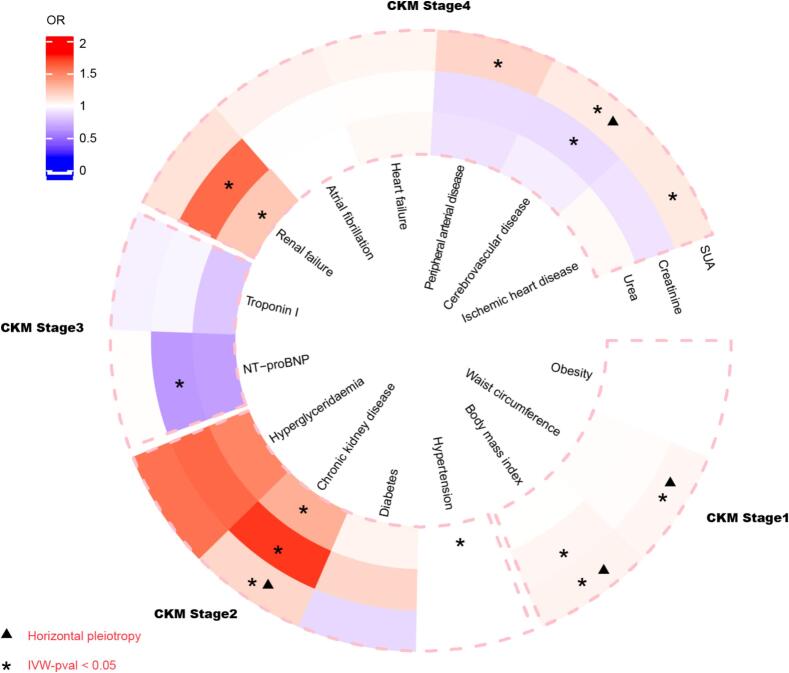
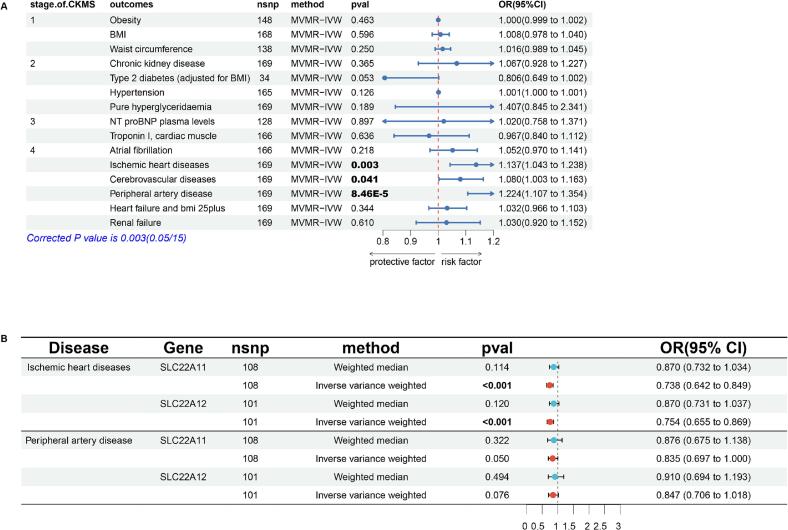
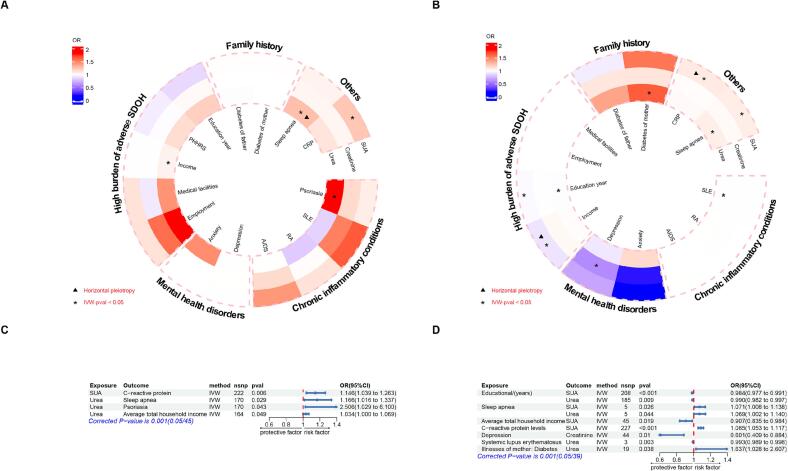
Regarding SUA, genetically predicted SUA demonstrated a potential risk effect on stage 4 of CKM syndrome (ischemic heart disease (IHD), OR = 1.090, 95 %CI: 1.003-1.184; peripheral artery disease, OR = 1.174, 95 %CI: 1.058-1.303). SUA remained a significant risk factor after excluding the confounding of eGFR and proteinuria (IHD: OR = 1.137, 95 %CI: 1.043-1.238; peripheral artery disease: OR = 1.224, 95 %CI: 1.107-1.354). SUA mediated the following causal effect: sleep apnea (2.37 %), income (1.92 %) and education (1.79 %) on IHD; C-reactive protein (11.65 %) and education (4.29 %) on peripheral artery disease. Regarding renal status, renal dysfunction led to a wider phenotype of CKM syndrome including hypertension, cerebrovascular disease, chronic kidney disease and renal failure. Similarly, renal status mediated the causal effect of education on hypertension (1.84 %), depression on cerebrovascular (0.46 %) and family history of diabetes on chronic kidney disease (3.49 %) and renal failure (2.81 %). Lesinurad targeting SLC22A11 and SLC22A12 was validated for treating IHD.
Our study clarified the complex relationship among SUA, renal status and CKM syndrome. Simultaneously providing innovative drug and social interventions for CKM syndrome.
血清尿酸(SUA)和肾脏状况与心血管-肾脏-代谢(CKM)综合征相关。然而,它们之间的因果关系以及药物治疗仍有待探索。
我们采用了单变量、多变量、中介和药物靶点孟德尔随机化方法。逆方差加权是主要结果,并进行了广泛的敏感性分析以确保稳健性和可靠性。
关于SUA,基因预测的SUA对CKM综合征4期(缺血性心脏病(IHD),OR = 1.090,95%CI:1.003 - 1.184;外周动脉疾病,OR = 1.174,95%CI:1.058 - 1.303)显示出潜在风险效应。排除估算肾小球滤过率(eGFR)和蛋白尿的混杂因素后,SUA仍然是一个显著的风险因素(IHD:OR = 1.137,95%CI:1.043 - 1.238;外周动脉疾病:OR = 1.224,95%CI:1.107 - 1.354)。SUA介导了以下因果效应:睡眠呼吸暂停(2.37%)、收入(1.92%)和教育程度(1.79%)对IHD的影响;C反应蛋白(11.65%)和教育程度(4.29%)对外周动脉疾病的影响。关于肾脏状况,肾功能不全导致CKM综合征的表型范围更广,包括高血压、脑血管疾病、慢性肾脏病和肾衰竭。同样,肾脏状况介导了教育程度对高血压(1.84%)、抑郁症对脑血管疾病(0.46%)以及糖尿病家族史对慢性肾脏病(3.49%)和肾衰竭(2.81%)的因果效应。靶向溶质载体家族成员22A11(SLC22A11)和溶质载体家族成员22A12(SLC22A12)的雷西纳德被证实可用于治疗IHD。
我们的研究阐明了SUA、肾脏状况和CKM综合征之间的复杂关系。同时为CKM综合征提供了创新的药物和社会干预措施。