Guo Ping, Zhang Ping, Zhao Jia Wei, Wang Amanda Y, Wang Wei
School of Medicine, University of Electronic Science and Technology of China, Chengdu, China.
Renal Department and Nephrology Institute, Sichuan Provincial People's Hospital, School of Medicine, University of Electronic Science and Technology of China, Chengdu, China.
Medicine (Baltimore). 2025 Aug 15;104(33):e43824. doi: 10.1097/MD.0000000000043824.
The coexistence of Guillain-Barré syndrome (GBS) and minimal change disease (MCD) is extremely rare. GBS is an autoimmune-mediated peripheral neuropathy that can occasionally be associated with renal complications such as nephrotic syndrome (NS). This case discusses a patient diagnosed with both GBS and MCD, as well as Sjögren syndrome kidney injury, focusing on the potential pathogenesis of these conditions and the role of autoantibodies in their development and treatment outcomes.
A young female patient presented with progressively worsening muscle weakness, sensory abnormalities, and edema. Further investigations revealed NS, characterized by proteinuria and hypoalbuminemia. While the neurological symptoms improved initially, the renal manifestations persisted, raising concerns about ongoing kidney damage. In addition, the patient was also found to have Sjögren syndrome kidney injury, along with positive perinuclear antineutrophil cytoplasmic antibody and antinuclear antibody, suggesting an autoimmune-mediated process contributing to the co-occurrence of these conditions.
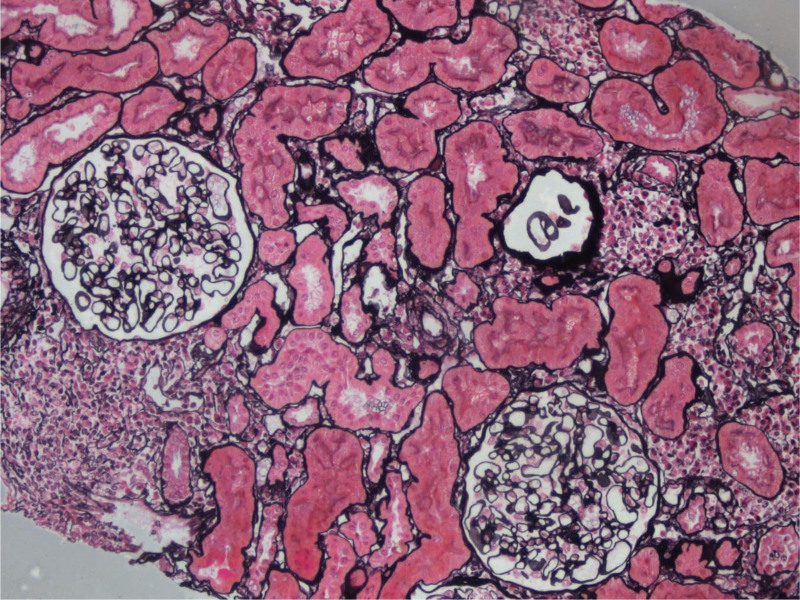
GBS was diagnosed based on characteristic ascending paralysis and demyelination, as evidenced by nerve conduction studies. The diagnosis of MCD was supported by the patient's clinical presentation of NS and kidney biopsy findings. The presence of clinical features such as dry mouth and dry eyes, coupled with positive anti-SSA/Ro52 and anti-Sjögren syndrome antigen B antibodies, pointed to Sjögren syndrome. Kidney biopsy results strongly suggested that kidney damage was likely due to Sjögren syndrome.
The patient was started on immunosuppressive therapy, including prednisone and cyclophosphamide, to address both the autoimmune neuropathy and renal issues. In addition, intravenous immunoglobulin was administered to treat the GBS. Supportive therapies, such as diuretics and albumin infusions, were used to manage edema and protein loss associated with NS.
The patient showed significant improvement in neurological symptoms, including enhanced muscle strength and reduced sensory deficits. Proteinuria decreased, and renal function gradually stabilized.
This case illustrates the rare coexistence of GBS, MCD, and Sjögren syndrome kidney injury in a single patient. Autoimmune markers played a pivotal role in the pathogenesis of these diseases. Immunosuppressive therapy and intravenous immunoglobulin were essential in treating both neurological and renal complications. Further research is needed to deepen our understanding of the overlap of autoimmune diseases and to optimize treatment strategies for such complex cases.
吉兰 - 巴雷综合征(GBS)与微小病变病(MCD)并存极为罕见。GBS是一种自身免疫介导的周围神经病变,偶尔可伴有肾病综合征(NS)等肾脏并发症。本病例讨论了一名同时诊断为GBS和MCD以及干燥综合征肾损伤的患者,重点关注这些病症的潜在发病机制以及自身抗体在其发生发展和治疗结果中的作用。
一名年轻女性患者出现进行性加重的肌肉无力、感觉异常和水肿。进一步检查发现NS,其特征为蛋白尿和低白蛋白血症。虽然神经症状最初有所改善,但肾脏表现持续存在,引发了对持续性肾损伤的担忧。此外,该患者还被发现患有干燥综合征肾损伤,同时核周型抗中性粒细胞胞浆抗体和抗核抗体呈阳性,提示自身免疫介导的过程导致了这些病症的共同发生。
根据特征性的上行性麻痹和脱髓鞘表现,通过神经传导研究确诊为GBS。患者NS的临床表现及肾活检结果支持MCD的诊断。口干、眼干等临床特征,以及抗SSA/Ro52和抗干燥综合征抗原B抗体阳性,提示干燥综合征。肾活检结果强烈提示肾损伤可能归因于干燥综合征。
患者开始接受免疫抑制治疗,包括泼尼松和环磷酰胺,以解决自身免疫性神经病变和肾脏问题。此外,给予静脉注射免疫球蛋白治疗GBS。使用利尿剂和白蛋白输注等支持性疗法来处理与NS相关的水肿和蛋白质丢失。
患者的神经症状有显著改善,包括肌肉力量增强和感觉缺陷减轻。蛋白尿减少,肾功能逐渐稳定。
本病例说明了GBS、MCD和干燥综合征肾损伤在单一患者中罕见的并存情况。自身免疫标志物在这些疾病的发病机制中起关键作用。免疫抑制治疗和静脉注射免疫球蛋白对于治疗神经和肾脏并发症至关重要。需要进一步研究以加深我们对自身免疫性疾病重叠的理解,并优化此类复杂病例的治疗策略。