Lu Jun, Yang Didi, Wang Yueying, Yang Shun, Fan Xiaohua, Bo Lulong
Department of Anesthesiology, Changhai Hospital, Naval Medical University, 168 Changhai Road, Shanghai, 200433, China.
BMC Anesthesiol. 2025 Aug 25;25(1):417. doi: 10.1186/s12871-025-03283-9.
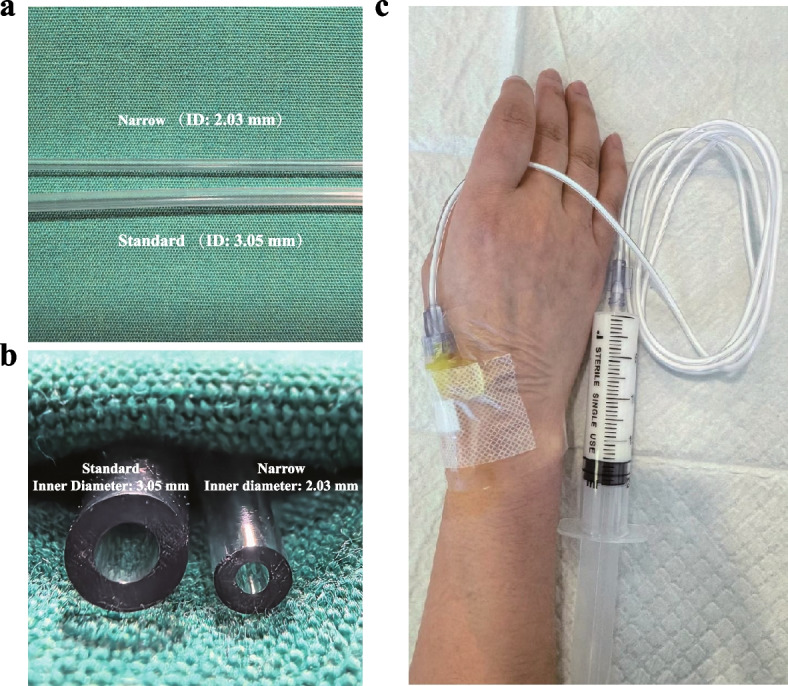
Hypoxemia is a common adverse event during propofol sedation for gastrointestinal endoscopy. Maintaining a sufficiently slow infusion rate is known to reduce respiratory depression caused by propofol, but achieving this consistently is challenging due to variations in manual techniques. This study evaluated the use of a narrow-bore extension tube to administer propofol, which passively slows infusion, to reduce hypoxemia during gastroscopy sedation.
A randomized controlled trial was conducted among patients undergoing propofol sedation for gastroscopy. Participants were assigned to either the narrow-bore extension tube group, which restricts infusion rates, or the control group receiving a standard-bore extension tube with unrestricted infusion rates. The primary outcome was the incidence of hypoxemia (SpO < 90%), with secondary outcomes including severe hypoxemia (SpO < 90% for ≥ 60 s or SpO < 75%), time to achieve deep sedation, total propofol dosage, and the incidence of pain on propofol injection (POPI). Subgroup analyses by age and BMI were performed.
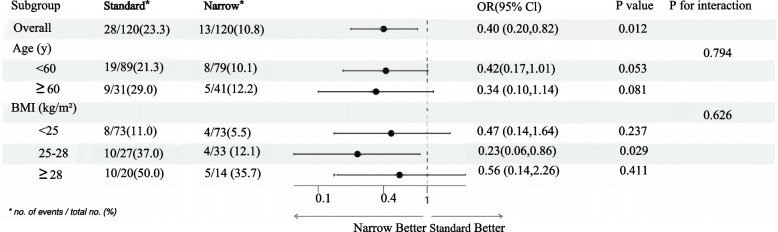
The incidence of hypoxemia was significantly lower in the narrow-bore extension tube (11.7% vs. 27.0%, p = 0.001), and there was a corresponding decrease in severe hypoxemia (7.3% vs. 19.7%, p = 0.003). The median time to achieve deep sedation was longer in the narrow-bore group (70 vs. 54 s; p < 0.001). The greatest reduction in hypoxemia was observed in overweight patients (BMI 25-28 kg/m, p = 0.029).
Using a narrow-bore extension tube to control propofol infusion rates significantly reduces hypoxemia during gastroscopy sedation. This cost-effective strategy is especially beneficial for higher-risk patients, such as those who are overweight.
The clinical trial was registered on Chinese Clinical Trial Register on December 16, 2024 (ChiCTR2400094042).
低氧血症是胃肠内镜检查丙泊酚镇静期间常见的不良事件。已知保持足够慢的输注速率可减少丙泊酚引起的呼吸抑制,但由于手动技术的差异,始终如一地做到这一点具有挑战性。本研究评估了使用细孔延长管输注丙泊酚,其可被动减慢输注速度,以减少胃镜检查镇静期间的低氧血症。
对接受丙泊酚镇静胃镜检查的患者进行了一项随机对照试验。参与者被分配到限制输注速率的细孔延长管组或接受输注速率不受限制的标准孔径延长管的对照组。主要结局是低氧血症(SpO₂<90%)的发生率,次要结局包括严重低氧血症(SpO₂<90%持续≥60秒或SpO₂<75%)、达到深度镇静的时间、丙泊酚总剂量以及丙泊酚注射时的疼痛发生率(POPI)。按年龄和BMI进行亚组分析。
细孔延长管组低氧血症的发生率显著更低(11.7%对27.0%,p = 0.001),严重低氧血症也相应减少(7.3%对19.7%,p = 0.003)。细孔组达到深度镇静的中位时间更长(70秒对54秒;p<0.001)。超重患者(BMI 25 - 28 kg/m²)的低氧血症减少最为明显(p = 0.029)。
使用细孔延长管控制丙泊酚输注速率可显著降低胃镜检查镇静期间的低氧血症。这种具有成本效益的策略对高危患者尤其有益,如超重患者。
该临床试验于2024年12月16日在中国临床试验注册中心注册(ChiCTR2400094042)。