Li Ning, Ou Wei, Cheng Chao, You Jian, Yang Lin, Chen Feng-Xia, Liang Yi, Yang Zhixiong, Wang Bao-Xiao, Chang Zeng-Hao, Lin Yao-Bin, Yang Weixiong, Xu Feng, Ding Guanggui, Chen Xian-Shan, Hu Ronggui, Li Shujun, Jiang Hao, Hu Xin-Xin, Long Hao, Wang Si-Yu
State Key Laboratory of Oncology in South China, Guangdong Provincial Clinical Research Center for Cancer, Sun Yat-sen University Cancer Center, Guangzhou, China.
The First Affiliated Hospital of Sun Yat-sen University, Guangzhou, China.
Signal Transduct Target Ther. 2025 Aug 28;10(1):273. doi: 10.1038/s41392-025-02358-w.
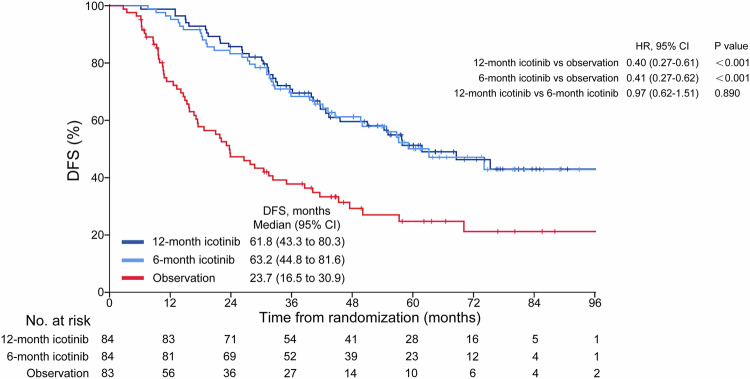
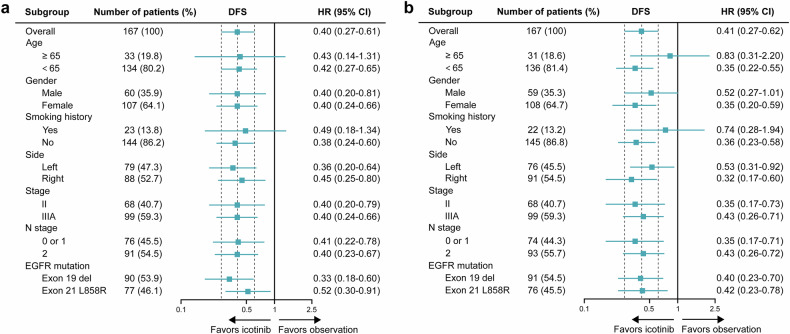
The efficacy, safety and ideal treatment duration of an adjuvant epidermal growth factor receptor tyrosine kinase inhibitor (EGFR-TKI) for patients with resected EGFR-mutated non-small-cell lung cancer (NSCLC) were not known until 2014, when this study was initiated. In this phase 3 ICTAN trial (GASTO1002, NCT01996098), patients with completely resected, EGFR-mutated, stage II-IIIA NSCLC after adjuvant chemotherapy were assigned in a 1:1:1 ratio to receive icotinib (125 mg, three times daily) for 12 months, to receive icotinib for 6 months, or to undergo observation. The primary endpoint was disease-free survival (DFS). This trial was terminated early. A total of 251 patients were randomized. Adjuvant icotinib for 12 months significantly improved DFS (hazard ratio [HR]: 0.40, 95% confidence interval [CI], 0.27-0.61; P < 0.001) and overall survival (OS; HR: 0.55, 95% CI, 0.32-0.96; P = 0.032) compared with observation. Adjuvant icotinib of 6 months also significantly improved DFS (HR: 0.41, 95% CI, 0.27-0.62; P < 0.001) and OS (HR: 0.56, 95% CI, 0.32-0.98; P = 0.038) compared with observation. Adjuvant icotinib for 12 months did not improve DFS (HR: 0.97; P = 0.89) or OS (HR: 1.00; P = 0.99) compared with 6 months of this drug. Rates of adverse events of grade 3 or higher were 8.3%, 6.0% and 2.4% for the 12-month icotinib, 6-month icotinib, and observation groups, respectively. Adjuvant icotinib for 12 months or 6 months following adjuvant chemotherapy improved DFS and OS compared with observation in patients with resected EGFR-mutated stage II-IIIA NSCLC with a manageable safety profile, supporting it as a potential treatment option.
在2014年启动这项研究之前,辅助性表皮生长因子受体酪氨酸激酶抑制剂(EGFR-TKI)用于接受手术切除的EGFR突变非小细胞肺癌(NSCLC)患者的疗效、安全性及理想治疗时长尚不清楚。在这项3期ICTAN试验(GASTO1002,NCT01996098)中,辅助化疗后完全切除、EGFR突变的II-IIIA期NSCLC患者按1:1:1比例分配,分别接受12个月的埃克替尼(125毫克,每日三次)治疗、接受6个月的埃克替尼治疗或接受观察。主要终点为无病生存期(DFS)。该试验提前终止。共有251例患者被随机分组。与观察相比,辅助使用12个月的埃克替尼显著改善了DFS(风险比[HR]:0.40,95%置信区间[CI],0.27 - 0.61;P < 0.001)和总生存期(OS;HR:0.55,95%CI,0.32 - 0.96;P = 0.032)。与观察相比,辅助使用6个月的埃克替尼也显著改善了DFS(HR:0.41,95%CI,0.27 - 0.62;P < 0.001)和OS(HR:0.56,95%CI,0.32 - 0.98;P = 0.038)。与使用6个月的该药相比,辅助使用12个月的埃克替尼未改善DFS(HR:0.97;P = 0.89)或OS(HR:1.00;P = 0.99)。3级及以上不良事件发生率在12个月埃克替尼组、6个月埃克替尼组和观察组分别为8.3%、6.0%和2.4%。辅助化疗后使用12个月或6个月的埃克替尼与观察相比,改善了接受手术切除的EGFR突变II-IIIA期NSCLC患者的DFS和OS,且安全性可控,支持其作为一种潜在的治疗选择。