Arthur Adam S, Jahromi Babak S, Saphier Paul S, Nickele Christopher M, Ryan Robert W, Vajkoczy Peter, Schirmer Clemens M, Kellner Christopher P, Matouk Charles C, Arias Eric J, Ullman Jamie S, Levitt Michael R, Hage Ziad A, Fiorella David J
Department of Neurosurgery, Semmes-Murphey Clinic and University of Tennessee Health Sciences Center, Memphis.
Department of Neurological Surgery, Northwestern Memorial Hospital, Northwestern University Feinberg School of Medicine, Chicago, Illinois.
JAMA Neurol. 2025 Sep 2. doi: 10.1001/jamaneurol.2025.3151.
It remains uncertain whether surgical evacuation improves functional outcomes in patients with supratentorial intracerebral hemorrhage (ICH).
To compare the safety and efficacy of minimally invasive surgery with the Artemis Neuro Evacuation Device to guideline-based medical management alone for spontaneous supratentorial ICH.
DESIGN, SETTING, AND PARTICIPANTS: The MIND open-label, multicenter randomized clinical trial randomized patients with spontaneous supratentorial ICH in a 2:1 ratio to either minimally invasive surgery or medical management alone. Participants were enrolled at 32 participating global sites between February 6, 2018, and August 28, 2023. This article reports on the primary trial outcome. Of 4066 eligible adult patients (aged 18-80 years) with moderate- to large-volume supratentorial ICH (20-80 mL), baseline National Institutes of Health Stroke Scale score of 6 or higher, and Glasgow Coma Scale score between 5 and 15, 154 were randomized to minimally invasive surgery and 82 to medical management. Data were analyzed from February to September 2024.
Minimally invasive surgery (within 72 hours of symptom onset) plus medical management or medical management alone.
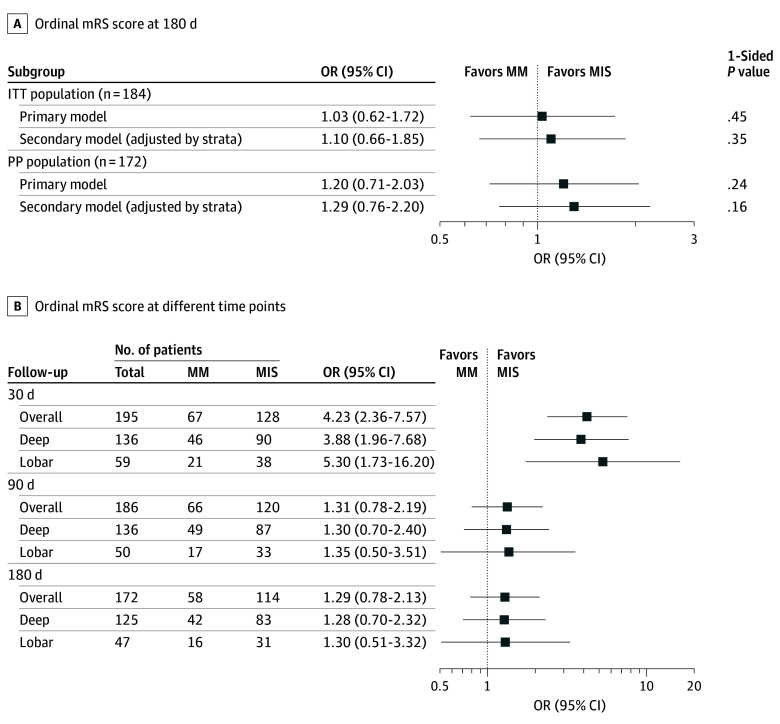
The primary efficacy outcome was 180-day combined death and disability via ordinal modified Rankin Scale score (range, 0 [no symptoms] to 6 [death]). The primary safety outcome was 30-day mortality.
Following an independent feasibility analysis prompted by the publication of positive results of a contemporaneous ICH trial, enrollment was stopped early at 236 participants. Overall median (IQR) participant age was 60 (50-70) years, 87 participants (36.9%) were female, 164 (69.5%) had primarily deep bleeds, and 72 (30.5%) had primarily lobar bleeds. Efficacy results of the primary model analysis suggested lack of evidence for the superiority of minimally invasive surgery over medical management (odds ratio [OR], 1.03; 96% CI, 0.62-1.72; P = .45). The adjusted model's mean OR was also nonsignificantly greater than 1 (OR, 1.10; 96% CI, 0.66-1.85; P = .35). By 30 days, 11 participants (7.2%) in the surgery group and 8 (9.8%) in the medical management group died (difference, -2.5%; 95% CI, -11.7% to 4.8%).
In the MIND randomized clinical trial, minimally invasive surgery within 72 hours did not significantly reduce 30-day mortality or improve 180-day disability in patients with supratentorial ICH compared to medical management alone.
ClinicalTrials.gov Identifier: NCT03342664.
幕上脑出血(ICH)患者手术清除血肿是否能改善功能预后仍不确定。
比较使用Artemis神经清除装置的微创手术与单纯基于指南的药物治疗对自发性幕上ICH的安全性和有效性。
设计、地点和参与者:MIND开放标签、多中心随机临床试验,将自发性幕上ICH患者按2:1的比例随机分为微创手术组或单纯药物治疗组。参与者于2018年2月6日至2023年8月28日在32个参与的全球研究地点入组。本文报告主要试验结果。在4066名符合条件的成年患者(年龄18 - 80岁)中,幕上中大量ICH(20 - 80 mL)、美国国立卫生研究院卒中量表基线评分6分或更高、格拉斯哥昏迷量表评分在5至15分之间,154名被随机分配至微创手术组,82名被分配至药物治疗组。数据于2024年2月至9月进行分析。
症状发作72小时内的微创手术加药物治疗或单纯药物治疗。
主要疗效结局是通过改良Rankin量表序数评分(范围为0[无症状]至6[死亡])评估的180天死亡和残疾合并情况。主要安全性结局是30天死亡率。
在一项同期ICH试验阳性结果发表引发的独立可行性分析后,236名参与者提前停止入组。参与者总体中位(四分位间距)年龄为60(50 - 70)岁,87名参与者(36.9%)为女性,164名(69.5%)主要为深部出血,72名(30.5%)主要为脑叶出血。主要模型分析的疗效结果表明,缺乏证据支持微创手术优于药物治疗(优势比[OR],1.03;96%置信区间,0.62 - 1.72;P = 0.45)。调整模型的平均OR也无显著大于1(OR,1.10;96%置信区间,0.66 - 1.85;P = 0.35)。到30天时,手术组11名参与者(7.2%)死亡,药物治疗组8名(9.8%)死亡(差异,-2.5%;95%置信区间,-11.7%至4.8%)。
在MIND随机临床试验中,与单纯药物治疗相比,72小时内的微创手术并未显著降低幕上ICH患者的30天死亡率或改善180天残疾情况。
ClinicalTrials.gov标识符:NCT03342664