Robinson Eric, Liu Tom, Malaisrie S Chris, Kruse Jane, Whippo Beth, An Seokyung, Baldridge Abigail S, Johnston Douglas R, Cox James L, McCarthy Patrick M, Pham Duc T, Mehta Christopher K
Division of Cardiac Surgery, Northwestern University Feinberg School of Medicine and Northwestern Medicine Bluhm Cardiovascular Institute, Chicago, Ill.
JTCVS Open. 2025 Jun 20;26:52-60. doi: 10.1016/j.xjon.2025.06.007. eCollection 2025 Aug.
Limited data are available on treatment of atrial fibrillation during ascending aortic aneurysm and aortic valve surgery. Ablation at the time of isolated aortic valve surgery has a Society of Thoracic Surgeons Class I indication. We sought to determine early and late outcomes of concomitant atrial fibrillation surgery at the time of ascending aortic aneurysm + aortic valve surgery.
From July 2008 to June 2023, patients undergoing elective ascending aortic aneurysm + aortic valve surgery ± atrial fibrillation surgery were compared. Clinical follow-up was conducted annually (median 5.6 [3.1-9.2] years).
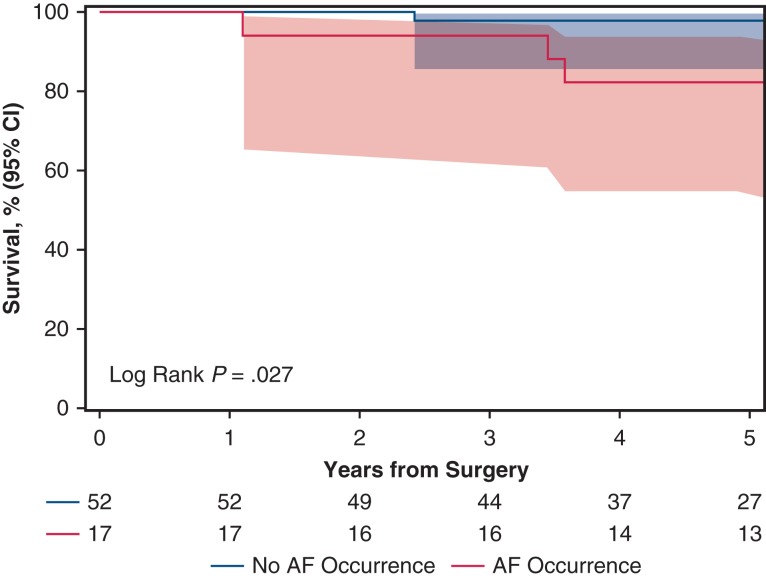
Of 792 patients in the cohort, 89 (11.2%) had preoperative atrial fibrillation and all underwent atrial fibrillation ablation procedures: pulmonary vein isolation (42.7%), left atrial cryoablation (19.1%), and biatrial cryoablation (38.2%). After 2:1 propensity score matching between the no atrial fibrillation (123) and ablation groups (67), postoperative complications were pacemaker implant (1.7% vs 1.6%; 952), new-onset dialysis (0.8% vs 3.0%, 251), and 30-day mortality (0.8% vs 1.5%, 661). In matched patients with no atrial fibrillation and atrial fibrillation surgery, overall survival at 1, 5, and 10 years was similar (4) at a mean of 6.22 years follow-up. Stroke incidence was similar at 7.8% versus 3.3% (236).
For patients undergoing aneurysm surgery concomitantly with aortic valve surgery, surgical ablation was effective and did not increase 30-day mortality. Survival and stroke outcomes were similar to a matched reference group without preoperative atrial fibrillation. Ablation of atrial fibrillation should be considered at the time of aortic surgery.
关于升主动脉瘤和主动脉瓣手术期间房颤治疗的数据有限。单纯主动脉瓣手术时进行消融有胸外科医师协会I类指征。我们试图确定升主动脉瘤 + 主动脉瓣手术时同期进行房颤手术的早期和晚期结果。
对2008年7月至2023年6月期间接受择期升主动脉瘤 + 主动脉瓣手术 ± 房颤手术的患者进行比较。每年进行临床随访(中位时间5.6 [3.1 - 9.2]年)。
在该队列的792例患者中,89例(11.2%)术前有房颤,均接受了房颤消融手术:肺静脉隔离(42.7%)、左心房冷冻消融(19.1%)和双心房冷冻消融(38.2%)。在无房颤组(123例)和消融组(67例)进行2:1倾向评分匹配后,术后并发症包括起搏器植入(1.7%对1.6%;P = 0.952)、新发透析(0.8%对3.0%,P = 0.251)和30天死亡率(0.8%对1.5%,P = 0.661)。在无房颤和进行房颤手术的匹配患者中,平均随访6.22年时,1年、5年和10年的总生存率相似(P = 0.4)。中风发生率相似,分别为7.8%和3.3%(P = 0.236)。
对于同时进行动脉瘤手术和主动脉瓣手术的患者,手术消融有效且未增加30天死亡率。生存和中风结果与术前无房颤的匹配参照组相似。主动脉手术时应考虑消融房颤。