Alhadeethi Anaam R, Terrance Steffy, Hassan Mohamed E, Ali Khalid Al
AL Qassimi Women's and Children's Hospital (AQWCH), Sharjah, United Arab Emirate. (Drs. Alhadeethi, Hassan, and Ali).
Consultant Pediatric Surgeon at AQWCH, Sharjah, United Arab Emirates. (Drs. Alhadeethi and Hassan).
CRSLS. 2025 Sep 17;12(3). doi: 10.4293/CRSLS.2025.00046. eCollection 2025 Jul-Sep.
Splenic cysts are rare lesions that are classified as either true (primary) or false (secondary) cysts based on their epithelial lining. The pathogenesis of primary splenic cysts is not well understood, and several hypotheses have been proposed, including the Mesothelial invagination theory, which postulates that during development, the mesothelial lining invades along with the capsule. As the lining has a pluripotent nature, it has the propensity to undergo metaplasia and secretion of fluid, leading to the formation of cysts.
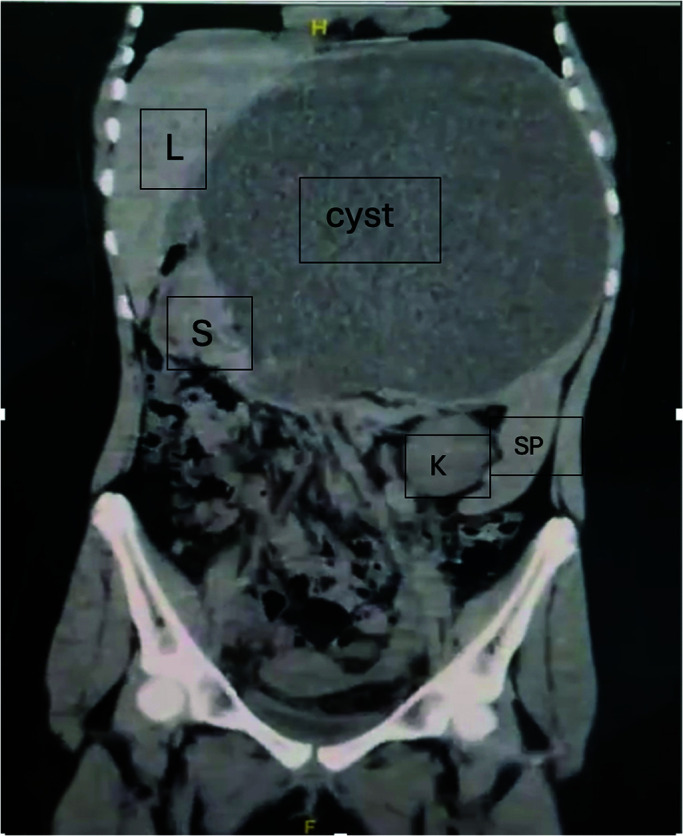
A 12-year-old female patient presented with a visible upper abdominal, painless cystic lesion, underwent blood tests and radiological diagnostic tools, such as abdominal ultrasound and computed tomography (CT) scan, but no definite diagnosis could be reached. Ultrasound-guided aspiration of the cyst was done, followed by explorative laparoscopy with total excision of the cyst (which was found to originate from the spleen), accompanied by partial splenectomy. The cyst was diagnosed as a benign primary mesothelial cyst of the spleen by histopathology. The patient experienced an uneventful postoperative period and showed no recurrence during follow-up.
A significant challenge for surgeons in terms of diagnosis, surgical planning, and managing intraoperative surprises is the difficulty in detecting the origin and nature of a large abdominal cyst, despite the availability of highly sophisticated diagnostic tools. Minimally invasive partial splenectomy in the pediatric age group is a feasible surgical intervention.
脾囊肿是罕见的病变,根据其上皮内衬可分为真性(原发性)或假性(继发性)囊肿。原发性脾囊肿的发病机制尚不清楚,已提出多种假说,包括间皮内陷理论,该理论假定在发育过程中,间皮内衬与包膜一起侵入。由于内衬具有多能性,它有发生化生和分泌液体的倾向,从而导致囊肿形成。
一名12岁女性患者出现上腹部可见的无痛性囊性病变,进行了血液检查以及腹部超声和计算机断层扫描(CT)等放射学诊断检查,但未能明确诊断。在超声引导下对囊肿进行了抽吸,随后进行了探索性腹腔镜检查并将囊肿(发现起源于脾脏)完全切除,同时进行了部分脾切除术。通过组织病理学诊断该囊肿为脾脏良性原发性间皮囊肿。患者术后恢复顺利,随访期间未出现复发。
尽管有高度复杂的诊断工具,但对于外科医生来说,在诊断、手术规划和应对术中意外情况方面,一个重大挑战是难以检测到大的腹部囊肿的起源和性质。在儿童年龄组中进行微创部分脾切除术是一种可行的手术干预措施。