Knight G
Postgrad Med J. 1973 Dec;49(578):845-54. doi: 10.1136/pgmj.49.578.845.
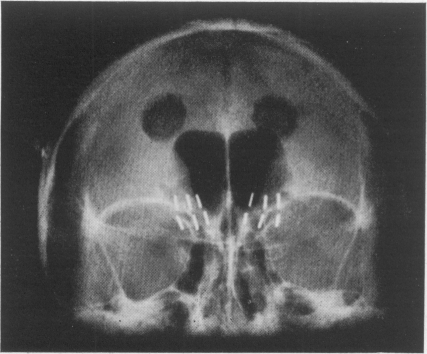
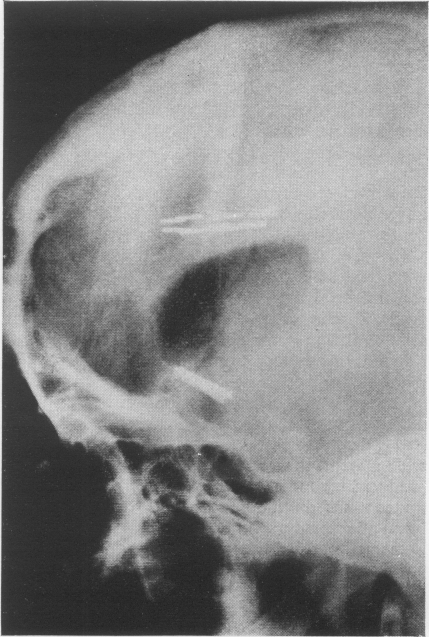
A study of the results of some 660 cases of stereotactic tractotomy shows that these have been consistent through a 12-year period, more than 50% of cases of resistant depression can be set free of medical care and another 25% at least can be improved. Comparable results are also obtained in obsessional illness and anxiety states, particularly those in which there is a depressive component. The original localization of the target site described in 1964 has not required modification but pathological studies and anatomical research has revealed new features concerning the anatomical connections affected by this operation. The lesion beneath the head of the caudate nucleus does not extend quite so far as the substantia innominata and should therefore be called subcaudate tractotomy. Connections from the anterior cingulate region and posterior orbital cortex are severed at this site but amygdalo-hypothalamic fibres are not interrupted directly, however; the projection from the amygdala to the dorsal median nucleus sends a radiation to the posterior orbital cortex which is divided here. In addition, important projections from frontal cortex to hypothalamus which bring the external milieu into association with the limbic system pass downwards through the target area beneath the head of the caudate nucleus and are also divided at this point, the localized lesion, therefore, produces a marked effect upon fibres which are concerned in emotional activity. The wellnigh specific effect in cases of depression raises the question whether the operation acts by modifying the intensity of emotional reactivity through limbic connections or has a more specific effect upon the cause of abnormal reactivity through fronto-hypothalamic connections exerting an influence on monoamine production in the hypothalamus.
一项对约660例立体定向束切断术结果的研究表明,这些结果在12年期间是一致的,超过50%的难治性抑郁症患者可以摆脱医疗护理,另外至少25%的患者病情可以得到改善。在强迫症和焦虑症状态中也获得了类似的结果,特别是那些伴有抑郁成分的疾病。1964年描述的靶点部位的原始定位无需修改,但病理研究和解剖学研究揭示了有关该手术所影响的解剖连接的新特征。尾状核头部下方的病变并没有延伸到无名质那么远,因此应称为尾状核下束切断术。在此部位,来自前扣带回区域和眶后皮质后部的连接被切断,但杏仁核-下丘脑纤维并没有直接中断;从杏仁核到背正中核的投射向眶后皮质后部发出一束纤维,在此处被分开。此外,从额叶皮质到下丘脑的重要投射将外部环境与边缘系统联系起来,这些投射向下穿过尾状核头部下方的靶点区域,也在此处被分开,因此,局部病变对参与情绪活动的纤维产生了显著影响。抑郁症病例中几乎具有特异性的效果提出了一个问题,即该手术是通过改变边缘系统连接的情绪反应强度起作用,还是通过额叶-下丘脑连接对下丘脑单胺产生施加影响,从而对异常反应的原因产生更具体的作用。