Andruss R J, Herndon J H
Department of Orthopaedic Surgery, University of Pittsburgh Medical Center, PA.
Iowa Orthop J. 1993;13:208-13.
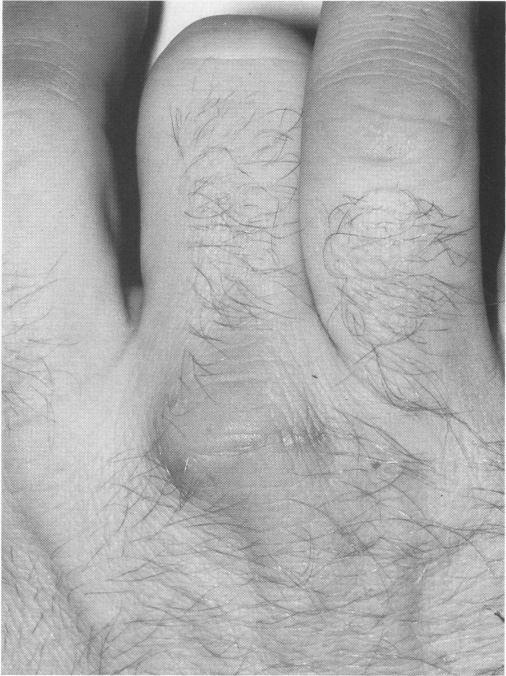
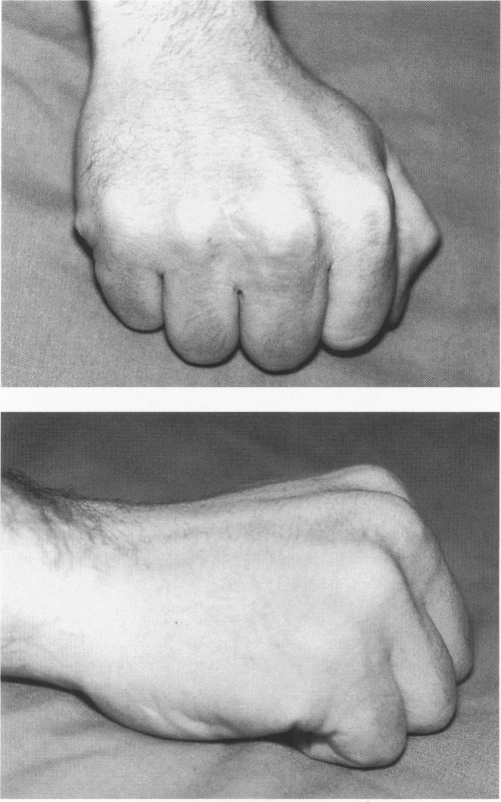
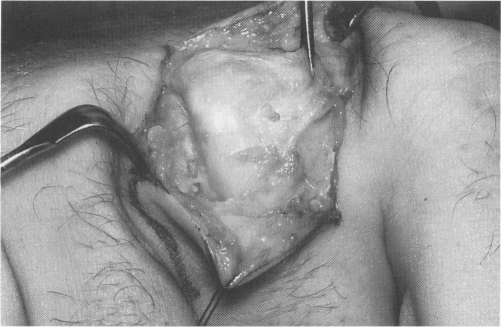
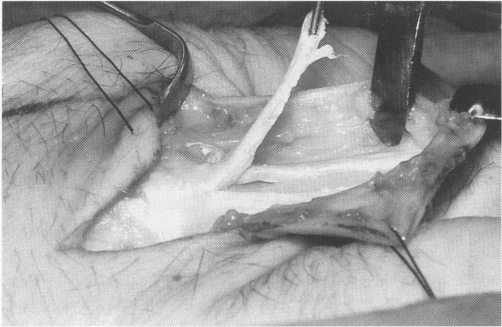
Ulnar subluxation of the extensor digitorum communis tendon at the MCP joint occurs infrequently in the nonrheumatoid patient and is secondary to one of four reported etiologies: traumatic, spontaneous, congenital, or epileptic. If symptomatic, patients may present with pain, swelling, a sensation of the tendon "snapping", "catching", "locking", or the inability to fully extend the MCP joint. Conservative and operative interventions have been recommended as treatment options. In the acute traumatic dislocation (less than ten days post injury), satisfactory results may be obtained with simple splinting with the MCP joint in extension. Patients who have failed conservative management or have a more chronic or degenerative dislocation may require surgical correction. The successful surgical repair must meet two requirements: (1) the tendon must be accurately aligned over the MCP joint to diminish the forces causing the dislocation to occur, and (2) the repair must be able to withstand the ulnar forces incurred during flexion of the joint. Realignment of the extensor tendon and direct repair of the radial sagittal band may be sufficient in acute traumatic, congenital, or spontaneous cases if the tissue is sufficient. In chronic dislocations or in cases with atrophic or degenerative tissue, reconstruction with augmentation of the radial restraints to the extensor hood is advised.
在非类风湿性患者中,指总伸肌腱在掌指关节处的尺侧半脱位很少见,其继发于四种已报道的病因之一:创伤性、自发性、先天性或癫痫性。如果出现症状,患者可能表现为疼痛、肿胀、肌腱“弹响”“卡顿”“绞锁”的感觉,或无法完全伸直掌指关节。保守治疗和手术干预均被推荐为治疗选择。在急性创伤性脱位(受伤后不到十天)时,将掌指关节伸直进行简单夹板固定可能会取得满意的效果。保守治疗失败或存在更慢性或退行性脱位的患者可能需要手术矫正。成功的手术修复必须满足两个要求:(1)肌腱必须在掌指关节上精确对齐,以减少导致脱位的力量;(2)修复必须能够承受关节屈曲时产生的尺侧力量。在急性创伤性、先天性或自发性病例中,如果组织足够,伸肌腱重新对齐并直接修复桡侧矢状带可能就足够了。在慢性脱位或组织萎缩或退变的病例中,建议通过增强伸肌帽的桡侧约束进行重建。