Beck J, Bohnet B, Brügger D, Bader P, Dietl J, Scheper R J, Kandolf R, Liu C, Niethammer D, Gekeler V
Children's Hospital, Tübingen, Germany.
Br J Cancer. 1998;77(1):87-91. doi: 10.1038/bjc.1998.13.
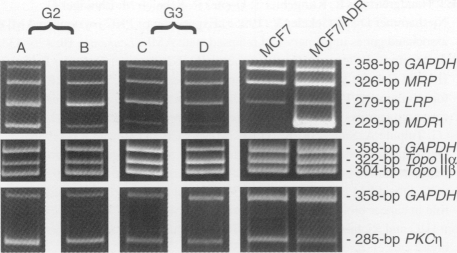
A possible link between protein kinase C (PKC) and P-glycoprotein (P-gp)-mediated-multidrug resistance (MDR) was assumed from studies on MDR cell lines selected in vitro. The functional relevance of PKC for the MDR phenotype remains unclear, and the involvement of a particular PKC isozyme in clinically occurring drug resistance is not known. Recently, we have demonstrated significant correlations between the expression levels of the PKC eta isozyme and the MDR1 or MRP (multidrug resistance-associated protein) genes in blasts from patients with acute myelogenous leukaemia (AML) and in ascites cell aspirates from ovarian cancer patients. To extend these findings to further types of human tumours we analysed specimens from 64 patients with primary breast cancer for their individual expression levels of several MDR-associated genes (MDR1, MRP, LRP (lung cancer resistance-related protein), topoisomerase (Topo) II alpha/IIbeta, cyclin A and the PKC isozyme genes (alpha, beta1, beta2, eta, theta, and mu) by a cDNA-PCR approach. We found significantly enhanced mean values for MRP, LRP and PKC eta gene expression, but significantly decreased Topo II alpha and cyclin A gene expression levels in G2 tumours compared with G3. Remarkably, significant positive correlations between the MDR1, MRP or LRP gene expression levels and PKC eta were determined: MDR1/PKC eta (rs = +0.6451, P < 0.0001) n = 62; MRP/PKC eta (rs = +0.5454, P < 0.0001) n = 63; LRP/PKC eta (rs = +0.5436, P < 0.0001) n = 62; MRP/LRP (rs = +0.7703, P < 0.0001) and n = 62, MDR1/MRP (rs = +0.5042, P < 0.0001) n = 62. Our findings point to the occurrence of a multifactorial MDR in the clinics and to PKC eta as a possible key regulatory factor for up-regulation of a series of MDR-associated genes in different types of tumours.
从对体外筛选出的多药耐药(MDR)细胞系的研究中推测,蛋白激酶C(PKC)与P-糖蛋白(P-gp)介导的多药耐药之间可能存在联系。PKC对MDR表型的功能相关性仍不清楚,且尚不清楚特定的PKC同工酶是否参与临床发生的耐药。最近,我们已经证实在急性髓性白血病(AML)患者的原始细胞以及卵巢癌患者的腹水细胞抽提物中,PKC η同工酶的表达水平与MDR1或多药耐药相关蛋白(MRP)基因之间存在显著相关性。为了将这些发现扩展到更多类型的人类肿瘤,我们采用cDNA-PCR方法分析了64例原发性乳腺癌患者标本中几种MDR相关基因(MDR1、MRP、肺癌耐药相关蛋白(LRP)、拓扑异构酶(Topo)IIα/IIβ、细胞周期蛋白A和PKC同工酶基因(α、β1、β2、η、θ和μ)的个体表达水平。我们发现,与G3期肿瘤相比,G2期肿瘤中MRP、LRP和PKC η基因表达的平均值显著升高,但Topo IIα和细胞周期蛋白A基因表达水平显著降低。值得注意的是,确定了MDR1、MRP或LRP基因表达水平与PKC η之间存在显著正相关:MDR1/PKC η(rs = +0.6451,P < 0.0001),n = 62;MRP/PKC η(rs = +0.5454,P < 0.0001),n = 63;LRP/PKC η(rs = +0.5436,P < 0.0001),n = 62;MRP/LRP(rs = +0.7703,P < 0.0001),n = 62,MDR1/MRP(rs = +0.5042,P < 0.0001),n = 62。我们的研究结果表明临床上存在多因素MDR,并且PKC η可能是不同类型肿瘤中一系列MDR相关基因上调的关键调节因子。