Kelly A, Ng D, Ferry R J, Grimberg A, Koo-McCoy S, Thornton P S, Stanley C A
Division of Endocrinology, The Children's Hospital of Philadelphia, and Department of Pediatrics, University of Pennsylvania School of Medicine, Philadelphia, Pennsylvania 19104, USA.
J Clin Endocrinol Metab. 2001 Aug;86(8):3724-8. doi: 10.1210/jcem.86.8.7755.
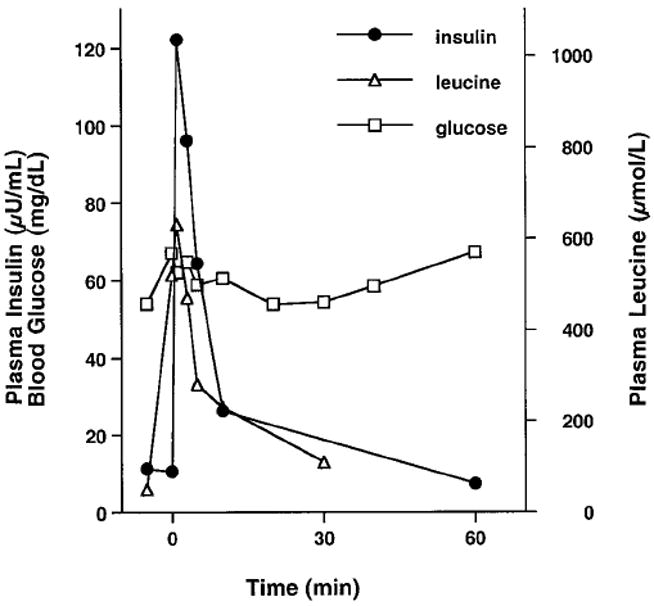
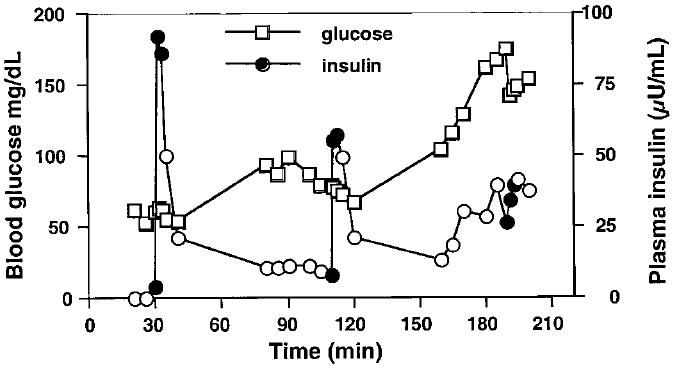
Mutations of glutamate dehydrogenase cause the hyperinsulinism/hyperammonemia syndrome by desensitizing glutamate dehydrogenase to allosteric inhibition by GTP. Normal allosteric activation of glutamate dehydrogenase by leucine is thus uninhibited, leading us to propose that children with hyperinsulinism/hyperammonemia syndrome will have exaggerated acute insulin responses to leucine in the postabsorptive state. As hyperglycemia increases beta-cell GTP, we also postulated that high glucose concentrations would extinguish abnormal responsiveness to leucine in hyperinsulinism/hyperammonemia syndrome patients. After an overnight fast, seven hyperinsulinism/hyperammonemia syndrome patients (aged 9 months to 29 yr) had acute insulin responses to leucine performed using an iv bolus of L-leucine (15 mg/kg) administered over 1 min and plasma insulin measurements obtained at -10, -5, 0, 1, 3, and 5 min. The acute insulin response to leucine was defined as the mean increase in insulin from baseline at 1 and 3 min after an iv leucine bolus. The hyperinsulinism/hyperammonemia syndrome group had excessively increased insulin responses to leucine (mean +/- SEM, 73 +/- 21 microIU/ml) compared with the control children and adults (n = 17) who had no response to leucine (1.9 +/- 2.7 microU/ml; P < 0.05). Four hyperinsulinism/hyperammonemia syndrome patients then had acute insulin responses to leucine repeated at hyperglycemia (blood glucose, 150-180 mg/dl). High blood glucose suppressed their abnormal baseline acute insulin responses to leucine of 180, 98, 47, and 28 microU/ml to 73, 0, 6, and 19 microU/ml, respectively. This suppression suggests that protein-induced hypoglycemia in hyperinsulinism/hyperammonemia syndrome patients may be prevented by carbohydrate loading before protein consumption.
谷氨酸脱氢酶突变通过使谷氨酸脱氢酶对GTP的变构抑制脱敏而导致高胰岛素血症/高氨血症综合征。因此,亮氨酸对谷氨酸脱氢酶的正常变构激活未受抑制,这使我们提出,高胰岛素血症/高氨血症综合征患儿在吸收后状态下对亮氨酸的急性胰岛素反应会增强。由于高血糖会增加β细胞内的GTP,我们还推测高血糖浓度会消除高胰岛素血症/高氨血症综合征患者对亮氨酸的异常反应性。禁食过夜后,7名高胰岛素血症/高氨血症综合征患者(年龄9个月至29岁)接受了对亮氨酸的急性胰岛素反应测试,通过静脉注射1分钟内给予15mg/kg的L-亮氨酸,并在-10、-5、0、1、3和5分钟时测量血浆胰岛素。对亮氨酸的急性胰岛素反应定义为静脉注射亮氨酸推注后1分钟和3分钟时胰岛素相对于基线的平均增加量。与对亮氨酸无反应的对照儿童和成人(n = 17)相比,高胰岛素血症/高氨血症综合征组对亮氨酸的胰岛素反应过度增加(平均值±标准误,73±21μU/ml)(1.9±2.7μU/ml;P < 0.05)。然后,4名高胰岛素血症/高氨血症综合征患者在高血糖状态下(血糖150 - 180mg/dl)重复进行对亮氨酸的急性胰岛素反应测试。高血糖将他们对亮氨酸的异常基线急性胰岛素反应分别从180、98、47和28μU/ml抑制至73、0、6和19μU/ml。这种抑制表明,在摄入蛋白质前进行碳水化合物负荷可能预防高胰岛素血症/高氨血症综合征患者蛋白质诱导的低血糖。