Kim H, Cheigh J S
Department of Internal Medicine, Sungkyunkwan University, School of Medicine, Kangbuk Samsung Hospital, Pyung-Dong, Jongro-Ku, Seoul 110-102, Korea.
Korean J Intern Med. 2001 Jun;16(2):98-104. doi: 10.3904/kjim.2001.16.2.98.
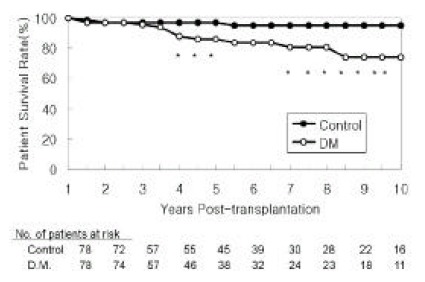
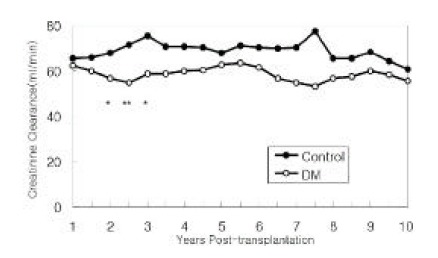
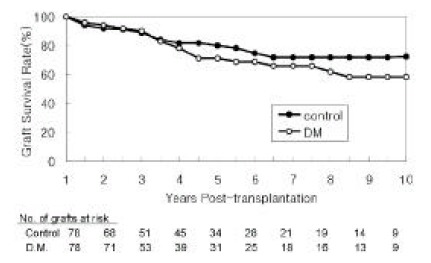
Kidney transplantation is the best therapeutic choice to improve survival and quality of life in patients with end-stage diabetic nephropathy. Long-term prognosis in diabetic patients who received kidney transplants, however, has not been delineated. We, therefore, studied patient and graft survival, graft function and cause of graft failure in 78 Type I diabetic kidney transplant recipients in The Rogosin Institute/The Weill-Cornell Medical Center, New York who had functioning grafts for more than one year. The results were compared with 78 non-diabetic patients who had functioning grafts for more than one year and were matched for age, gender, donor source, time of transplantation and immunosuppressive therapy protocol. Cumulative patient survival rates for diabetic patients were significantly lower than those of non-diabetic patients (86% vs. 97% at 5 years and 74% vs. 95% at 10 years, respectively; p < 0.05). The most common cause of death was cardiovascular disease. Graft survival rates for diabetic patients were also lower than that of non-diabetic patients (71% vs. 80% at 5 years and 58% vs. 72% at 10 years, respectively), but the differences did not reach statistical significance. Among the 22 failed grafts in diabetic patients, 7 (32%) were due to patient death rather than primary graft failure. If the patients who died with a functioning graft were censored, graft survival rates of diabetic patients approached those of non-diabetic patients (80% vs. 81% at 5 years and 65% vs. 73% at 10 years, respectively). Creatinine clearances in diabetic patients were lower than that in non-diabetic patients through the follow-up period, but the differences were significant only for the first few years. At no time was there a higher creatinine clearance for diabetic patients. Among the 16 patients who had transplant kidney biopsies two to seven years post-transplant, 6 showed morphological changes consistent with diabetic nephropathy. One patient lost graft function solely by recurrent diabetic nephropathy. We conclude that long-term patient survival for diabetic patients is significantly lower than that of non-diabetic patients, due primarily to cardiovascular disease. Graft survival is comparable between the two groups. Creatinine clearances of diabetic patients are lower than those of non-diabetic patients. There is no apparent glomerular hyperfiltration at any time in diabetic patients. Recurrence of diabetic nephropathy is a rare cause of graft failure in the first 10 year post-transplant period. Aggressive intervention to modify cardiovascular risk factors should improve patient and graft survival in diabetic kidney transplant recipients.
肾移植是改善终末期糖尿病肾病患者生存率和生活质量的最佳治疗选择。然而,接受肾移植的糖尿病患者的长期预后尚未明确。因此,我们研究了纽约罗戈辛研究所/威尔康奈尔医学院78例移植肾功能正常超过1年的I型糖尿病肾移植受者的患者和移植物存活率、移植物功能及移植物失功原因。将结果与78例移植肾功能正常超过1年且在年龄、性别、供体来源、移植时间和免疫抑制治疗方案方面相匹配的非糖尿病患者进行比较。糖尿病患者的累积患者生存率显著低于非糖尿病患者(5年时分别为86%对97%,10年时分别为74%对95%;p<0.05)。最常见的死亡原因是心血管疾病。糖尿病患者的移植物存活率也低于非糖尿病患者(5年时分别为71%对80%,10年时分别为58%对72%),但差异未达到统计学意义。在糖尿病患者的22例失功移植物中,7例(32%)是由于患者死亡而非原发性移植物失功。如果对移植肾功能正常时死亡的患者进行删失处理,糖尿病患者的移植物存活率接近非糖尿病患者(5年时分别为80%对81%,10年时分别为65%对73%)。在随访期间,糖尿病患者的肌酐清除率低于非糖尿病患者,但仅在最初几年差异有统计学意义。糖尿病患者在任何时候都没有更高的肌酐清除率。在移植后2至7年进行移植肾活检的16例患者中,6例显示出与糖尿病肾病一致的形态学改变。1例患者仅因复发性糖尿病肾病而失去移植物功能。我们得出结论,糖尿病患者的长期患者生存率显著低于非糖尿病患者,主要原因是心血管疾病。两组间移植物存活率相当。糖尿病患者的肌酐清除率低于非糖尿病患者。糖尿病患者在任何时候都没有明显的肾小球高滤过。糖尿病肾病复发是移植后最初10年内移植物失功的罕见原因。积极干预以改变心血管危险因素应能提高糖尿病肾移植受者的患者和移植物存活率。