Stieb David M, De Civita Paul, Johnson F Reed, Manary Matthew P, Anis Aslam H, Beveridge Robert C, Judek Stan
Healthy Environments and Consumer Safety Branch, Health Canada, Ottawa, ON, Canada.
Environ Health. 2002 Dec 18;1(1):7. doi: 10.1186/1476-069x-1-7.
Few assessments of the costs and benefits of reducing acute cardiorespiratory morbidity related to air pollution have employed a comprehensive, explicit approach to capturing the full societal value of reduced morbidity.
We used empirical data on the duration and severity of episodes of cardiorespiratory disease as inputs to complementary models of cost of treatment, lost productivity, and willingness to pay to avoid acute cardiorespiratory morbidity outcomes linked to air pollution in epidemiological studies. A Monte Carlo estimation procedure was utilized to propagate uncertainty in key inputs and model parameters.
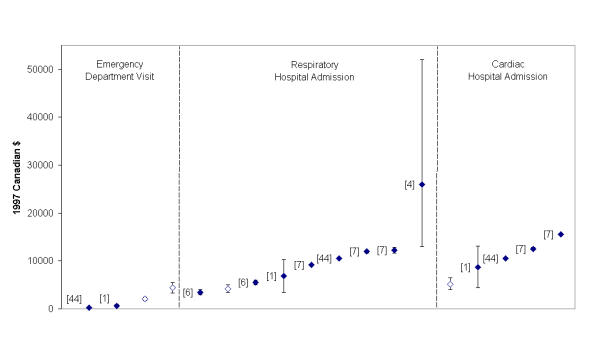
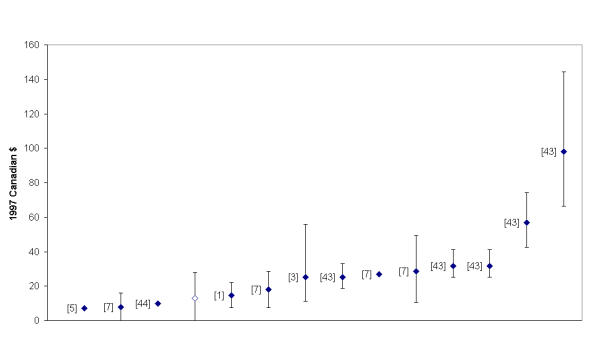
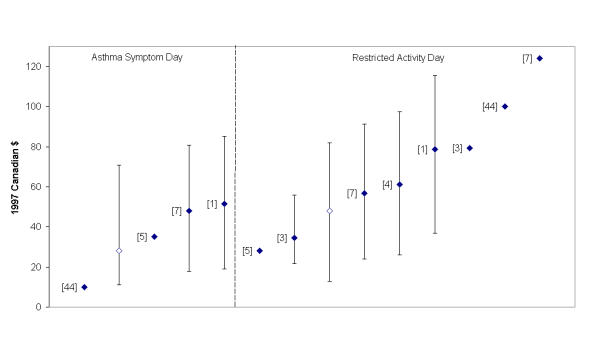
Valuation estimates ranged from 13 dollars (1997, Canadian) (95% confidence interval, 0-28 dollars) for avoidance of an acute respiratory symptom day to 5,200 dollars (4,000 dollars-6,400 dollars) for avoidance of a cardiac hospital admission. Cost of treatment accounted for the majority of the overall value of cardiac and respiratory hospital admissions as well as cardiac emergency department visits, while lost productivity generally represented a small proportion of overall value. Valuation estimates for days of restricted activity, asthma symptoms and acute respiratory symptoms were sensitive to alternative assumptions about level of activity restriction. As an example of the application of these values, we estimated that the observed decrease in particulate sulfate concentrations in Toronto between 1984 and 1999 resulted in annual benefits of 1.4 million dollars (95% confidence interval 0.91-1.8 million dollars) in relation to reduced emergency department visits and hospital admissions for cardiorespiratory disease.
Our approach to estimating the value of avoiding a range of acute morbidity effects of air pollution addresses a number of limitations of the current literature, and is applicable to future assessments of the benefits of improving air quality.
很少有关于降低与空气污染相关的急性心肺疾病发病率的成本效益评估采用全面、明确的方法来衡量发病率降低所带来的全部社会价值。
我们将心肺疾病发作的持续时间和严重程度的实证数据作为输入,用于治疗成本、生产力损失以及为避免流行病学研究中与空气污染相关的急性心肺疾病发病结果而支付意愿的补充模型。采用蒙特卡罗估计程序来传播关键输入和模型参数中的不确定性。
估值估计范围从避免一天急性呼吸道症状的13加元(1997年,加拿大)(95%置信区间,0 - 28加元)到避免一次心脏住院的5200加元(4000加元 - 6400加元)。治疗成本占心脏和呼吸住院以及心脏急诊科就诊总价值的大部分,而生产力损失通常占总价值的一小部分。对活动受限天数、哮喘症状和急性呼吸道症状的估值估计对活动受限水平的替代假设很敏感。作为这些值应用的一个例子,我们估计,1984年至1999年多伦多观察到的颗粒硫酸盐浓度下降导致与心肺疾病急诊科就诊和住院减少相关的年度效益为140万美元(95%置信区间0.91 - 180万美元)。
我们估计避免空气污染一系列急性发病影响价值的方法解决了当前文献中的一些局限性,适用于未来改善空气质量效益的评估。