Rocktaeschel Jens, Morimatsu Hiroshi, Uchino Shigehiko, Goldsmith Donna, Poustie Stephanie, Story David, Gutteridge Geoffrey, Bellomo Rinaldo
Department of Intensive Care and Department of Medicine, University of Melbourne, Australia.
Crit Care. 2003 Aug;7(4):R60. doi: 10.1186/cc2333. Epub 2003 Jun 4.
The aim of the present study is to understand the nature of acid-base disorders in critically ill patients with acute renal failure (ARF) using the biophysical principles described by Stewart and Figge. A retrospective controlled study was carried out in the intensive care unit of a tertiary hospital.
Forty patients with ARF, 40 patients matched for Acute Physiology and Chronic Health Evaluation II score (matched control group), and 60 consecutive critically ill patients without ARF (intensive care unit control group) participated. The study involved the retrieval of biochemical data from computerized records, quantitative biophysical analysis using the Stewart-Figge methodology, and statistical comparison between the three groups. We measured serum sodium, potassium, magnesium, chloride, bicarbonate, phosphate, ionized calcium, albumin, lactate and arterial blood gases.
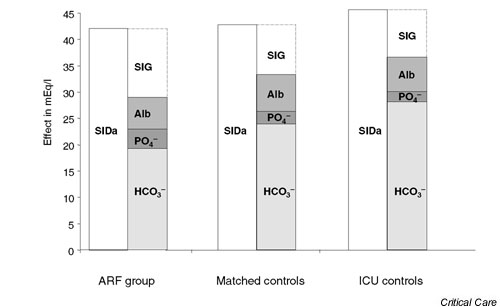
Intensive care unit patients with ARF had a mild acidemia (mean pH 7.30 +/- 0.13) secondary to metabolic acidosis with a mean base excess of -7.5 +/- 7.2 mEq/l. However, one-half of these patients had a normal anion gap. Quantitative acid-base assessment (Stewart-Figge methodology) revealed unique multiple metabolic acid-base processes compared with controls, which contributed to the overall acidosis. The processes included the acidifying effect of high levels of unmeasured anions (13.4 +/- 5.5 mEq/l) and hyperphosphatemia (2.08 +/- 0.92 mEq/l), and the alkalinizing effect of hypoalbuminemia (22.6 +/- 6.3 g/l).
The typical acid-base picture of ARF of critical illness is metabolic acidosis. This acidosis is the result of the balance between the acidifying effect of increased unmeasured anions and hyperphosphatemia and the lesser alkalinizing effect of hypoalbuminemia.
本研究的目的是运用斯图尔特(Stewart)和菲格(Figge)所描述的生物物理原理,了解急性肾衰竭(ARF)危重症患者酸碱紊乱的本质。在一家三级医院的重症监护病房开展了一项回顾性对照研究。
40例急性肾衰竭患者、40例急性生理与慢性健康状况评分系统II(APACHE II)评分匹配的患者(匹配对照组)以及60例连续入住重症监护病房且无急性肾衰竭的危重症患者(重症监护病房对照组)参与了研究。该研究包括从计算机记录中检索生化数据、使用斯图尔特 - 菲格方法进行定量生物物理分析以及三组之间的统计学比较。我们测量了血清钠、钾、镁、氯、碳酸氢盐、磷酸盐、离子钙、白蛋白、乳酸和动脉血气。
重症监护病房的急性肾衰竭患者继发于代谢性酸中毒,存在轻度酸血症(平均pH值7.30±0.13),平均碱剩余为 -7.5±7.2 mEq/L。然而,这些患者中有一半阴离子间隙正常。与对照组相比,定量酸碱评估(斯图尔特 - 菲格方法)显示存在独特的多种代谢性酸碱过程,这些过程导致了总体酸中毒。这些过程包括高水平未测定阴离子(13.4±5.5 mEq/L)和高磷血症(2.08±0.92 mEq/L)的酸化作用,以及低白蛋白血症(22.6±6.3 g/L)的碱化作用。
危重症急性肾衰竭的典型酸碱情况是代谢性酸中毒。这种酸中毒是未测定阴离子增加和高磷血症的酸化作用与低白蛋白血症较弱的碱化作用之间平衡的结果。