Ferreri A J M, Guerra E, Regazzi M, Pasini F, Ambrosetti A, Pivnik A, Gubkin A, Calderoni A, Spina M, Brandes A, Ferrarese F, Rognone A, Govi S, Dell'Oro S, Locatelli M, Villa E, Reni M
Department of Radiochemotherapy, San Raffaele H Scientific Institute, Via Olgettina 60, Milan 20132, Italy.
Br J Cancer. 2004 Jan 26;90(2):353-8. doi: 10.1038/sj.bjc.6601472.
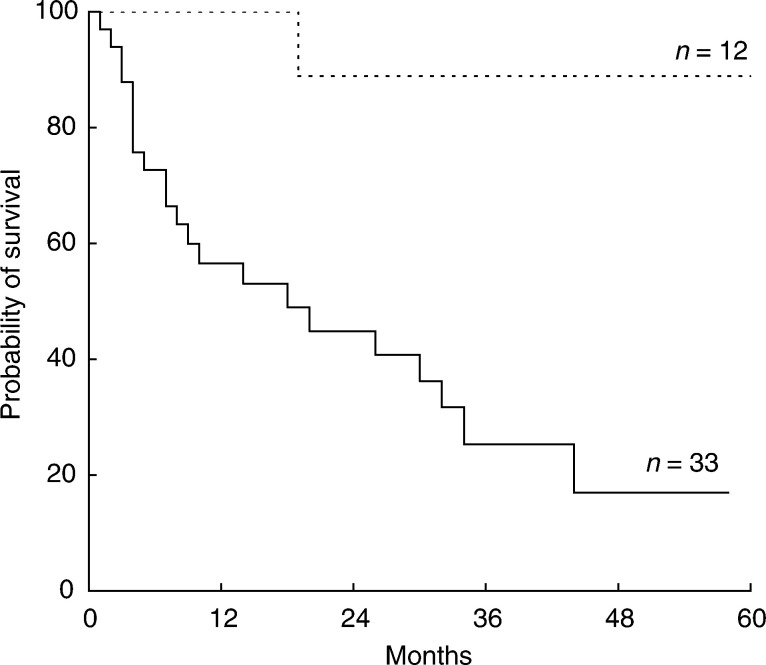
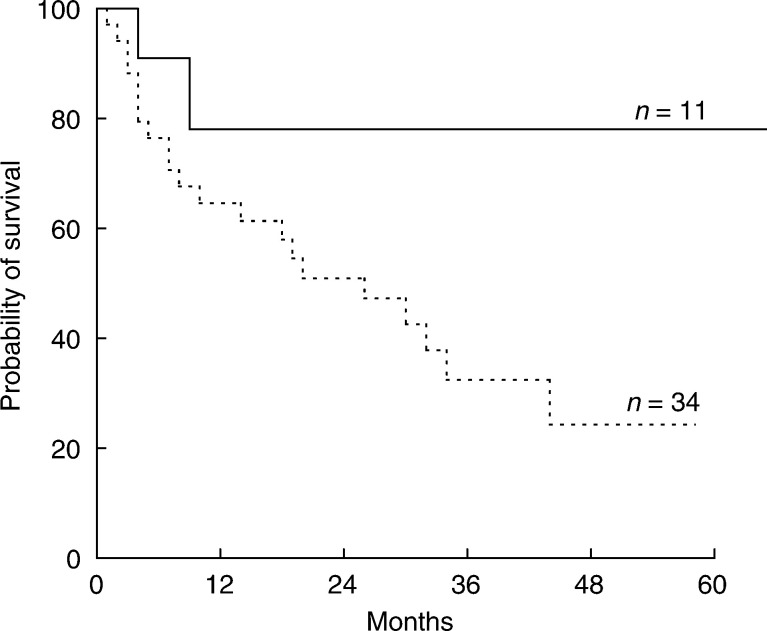
Although high-dose methotrexate (HD-MTX) is the most effective drug against primary CNS lymphomas (PCNSL), outcome-determining variables related to its administration schedule have not been defined. The impact on toxicity and outcome of the area under the curve (AUC(MTX)), dose intensity (DI(MTX)) and infusion rate (IR(MTX)) of MTX and plasmatic creatinine clearance (CL(crea)) was investigated in a retrospective series of 45 PCNSL patients treated with three different HD-MTX-based combinations. Anticonvulsants were administered in 31 pts (69%). Age >60 years, anticonvulsant therapy, slow IR(MTX) (</=800 mgm(-2)h(-1)), and reduced DI(MTX) (</=1000 mgm(-2)wk(-1)) were significantly correlated with low AUC(MTX) values. Seven patients (16%) experienced severe toxicity, which was independently associated with slow CL(crea). A total of 18 (40%) patients achieved complete remission after chemotherapy, which was independently associated with slow CL(crea). In all, 22 patients were alive at a median follow-up of 31 months, with a 3-year OS of 40+/-9%; slow CL(crea) and AUC(MTX) >1100 micromol hl(-1) were independently associated with a better survival. Slow CL(crea) and high AUC(MTX) are favourable outcome-determining factors in PCNSL, while slow CL(crea) is significantly related to higher toxicity. AUC(MTX) significantly correlates with age, anticonvulsant therapy, IR(MTX), and DI(MTX). These findings, which seem to support the choice of an MTX dose >/=3 gm(-2) in a 4-6-h infusion, every 3-4 weeks, deserve to be assessed prospectively in future trials. MTX dose adjustments in patients with fast CL(crea) should be investigated.
尽管大剂量甲氨蝶呤(HD-MTX)是治疗原发性中枢神经系统淋巴瘤(PCNSL)最有效的药物,但其给药方案中与预后相关的决定因素尚未明确。我们对45例接受三种不同的基于HD-MTX联合方案治疗的PCNSL患者进行了回顾性研究,探讨了甲氨蝶呤的曲线下面积(AUC(MTX))、剂量强度(DI(MTX))、输注速率(IR(MTX))以及血浆肌酐清除率(CL(crea))对毒性和预后的影响。31例患者(69%)接受了抗惊厥治疗。年龄>60岁、抗惊厥治疗、缓慢的IR(MTX)(≤800 mgm(-2)h(-1))以及降低的DI(MTX)(≤1000 mgm(-2)wk(-1))与低AUC(MTX)值显著相关。7例患者(16%)出现严重毒性反应,这与CL(crea)缓慢独立相关。共有18例(40%)患者化疗后达到完全缓解,这与CL(crea)缓慢独立相关。总体而言,22例患者在中位随访31个月时存活,3年总生存率为40±9%;CL(crea)缓慢和AUC(MTX)>1100 micromol hl(-1)与更好的生存率独立相关。CL(crea)缓慢和高AUC(MTX)是PCNSL中预后的有利决定因素,而CL(crea)缓慢与更高的毒性显著相关。AUC(MTX)与年龄、抗惊厥治疗、IR(MTX)和DI(MTX)显著相关。这些发现似乎支持每3 - 4周进行一次4 - 6小时输注、甲氨蝶呤剂量≥3 gm(-2)的选择,值得在未来试验中进行前瞻性评估。应研究CL(crea)快速的患者中甲氨蝶呤剂量调整情况。