Hogg William, Baskerville Neill, Lemelin Jacques
Department of Family Medicine, University of Ottawa, Canada.
BMC Health Serv Res. 2005 Mar 9;5(1):20. doi: 10.1186/1472-6963-5-20.
Outreach facilitation has been proven successful in improving the adoption of clinical preventive care guidelines in primary care practice. The net costs and savings of delivering such an intensive intervention need to be understood. We wanted to estimate the proportion of a facilitation intervention cost that is offset and the potential for savings by reducing inappropriate screening tests and increasing appropriate screening tests in 22 intervention primary care practices affecting a population of 90,283 patients.
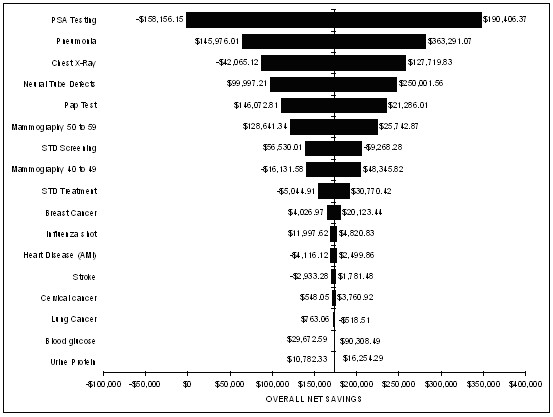
A cost-consequences analysis of one successful outreach facilitation intervention was done, taking into account the estimated cost savings to the health system of reducing five inappropriate tests and increasing seven appropriate tests. Multiple data sources were used to calculate costs and cost savings to the government. The cost of the intervention and costs of performing appropriate testing were calculated. Costs averted were calculated by multiplying the number of tests not performed as a result of the intervention. Further downstream cost savings were determined by calculating the direct costs associated with the number of false positive test follow-ups avoided. Treatment costs averted as a result of increasing appropriate testing were similarly calculated.
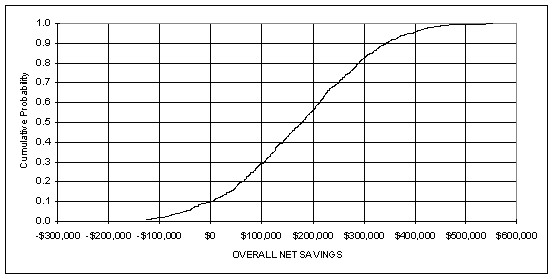
The total cost of the intervention over 12 months was $238,388 and the cost of increasing the delivery of appropriate care was $192,912 for a total cost of $431,300. The savings from reduction in inappropriate testing were $148,568 and from avoiding treatment costs as a result of appropriate testing were $455,464 for a total savings of $604,032. On a yearly basis the net cost saving to the government is $191,733 per year (2003 Can dollars) equating to $3,687 per physician or $63,911 per facilitator, an estimated return on intervention investment and delivery of appropriate preventive care of 40%.
Outreach facilitation is more expensive but more effective than other attempts to modify primary care practice and all of its costs can be offset through the reduction of inappropriate testing and increasing appropriate testing. Our calculations are based on conservative assumptions. The potential for savings is likely considerably higher.
已证实外展促进在改善基层医疗实践中临床预防保健指南的采用方面是成功的。需要了解提供这种强化干预的净成本和节省情况。我们希望估计在影响90283名患者的22家干预基层医疗实践中,促进干预成本被抵消的比例以及通过减少不适当筛查测试和增加适当筛查测试实现节省的潜力。
对一项成功的外展促进干预进行了成本-后果分析,考虑了减少五项不适当测试和增加七项适当测试给卫生系统带来的估计成本节省。使用多个数据源来计算政府的成本和成本节省。计算了干预成本和进行适当测试的成本。通过将因干预而未进行的测试数量相乘来计算避免的成本。通过计算与避免的假阳性测试后续数量相关的直接成本来确定进一步的下游成本节省。类似地计算因增加适当测试而避免的治疗成本。
12个月内干预的总成本为238388美元,增加适当护理的提供成本为192912美元,总成本为431300美元。减少不适当测试节省的费用为148568美元,因适当测试避免的治疗成本为455464美元,总节省为604032美元。每年政府的净成本节省为每年191733加元(2003年加拿大元),相当于每位医生3687加元或每位促进者63911加元,干预投资和提供适当预防保健的估计回报率为40%。
外展促进比其他改变基层医疗实践的尝试成本更高但更有效,并且其所有成本都可以通过减少不适当测试和增加适当测试来抵消。我们的计算基于保守假设。节省的潜力可能会高得多。