Vrbova Linda, Mamdani Muhammad, Moineddin Rahim, Jaakimainen Liisa, Upshur Ross E G
Department of Public Health Sciences, University of Toronto, McMurrich Building, 12 Queen's Park Crescent W, Toronto, ON, M5S 1A8, Canada.
J Negat Results Biomed. 2005 Apr 8;4:4. doi: 10.1186/1477-5751-4-4.
Low socioeconomic status has been associated with increased morbidity and mortality for various health conditions. The purpose of this study was twofold: to examine the mortality experience of older persons admitted to hospital with community acquired pneumonia and to test the hypothesis of whether an association exists between socioeconomic status and mortality subsequent to hospital admission for community-acquired pneumonia.
A population based retrospective cohort study was conducted including all older persons patients admitted to Ontario hospitals with community acquired pneumonia between April 1995 and March 2001. The main outcome measures were 30 day and 1 year mortality subsequent to hospital admission for community-acquired pneumonia.
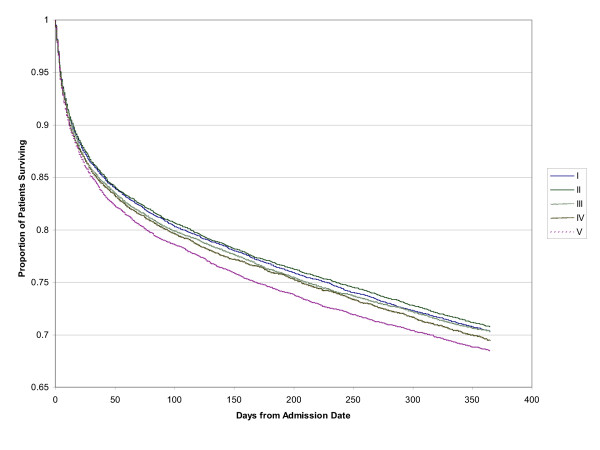
Socioeconomic status for each patient was imputed from median neighbourhood income. Multivariate analyses were undertaken to adjust for age, sex, co-morbid illness, hospital and physician characteristics. The study sample consisted of 60,457 people. Increasing age, male gender and high co-morbidity increased the risk for mortality at 30 days and one year. Female gender and having a family physician as attending physician reduced mortality risk. The adjusted odds of death after 30-days for the quintiles compared to the lowest income quintile (quintile 1) were 1.02 (95% CI: 0.95-1.09) for quintile 2, 1.04 (95% CI: 0.97-1.12) for quintile 3, 1.01 (95% CI: 0.94-1.08) for quintile 4 and 1.03 (95% CI: 0.96-1.12) for the highest income quintile (quintile 5). For 1 year mortality, compared to the lowest income quintile the adjusted odds ratios were 1.01 (95% CI: 0.96-1.06) for quintile 2, 0.99 (95% CI: 0.94-1.04) for quintile 3, 0.99 (95% CI: 0.93-1.05) for quintile 4 and 1.03 (95% CI: 0.97-1.10) for the highest income quintile.
Socioeconomic status is not associated with mortality in the older persons from community-acquired pneumonia in Ontario, Canada.
社会经济地位低下与多种健康状况下发病率和死亡率的增加有关。本研究有两个目的:研究因社区获得性肺炎入院的老年人的死亡情况,并检验社会经济地位与社区获得性肺炎入院后死亡率之间是否存在关联这一假设。
进行了一项基于人群的回顾性队列研究,纳入了1995年4月至2001年3月期间因社区获得性肺炎入住安大略省医院的所有老年患者。主要结局指标是社区获得性肺炎入院后的30天和1年死亡率。
根据邻里收入中位数估算每位患者的社会经济地位。进行多变量分析以调整年龄、性别、合并疾病、医院和医生特征。研究样本包括60457人。年龄增加、男性以及高合并症增加了30天和1年时的死亡风险。女性以及由家庭医生作为主治医生可降低死亡风险。与最低收入五分位数(五分位数1)相比,五分位数2在30天后的调整死亡比值比为1.02(95%可信区间:0.95-1.09),五分位数3为1.04(95%可信区间:0.97-1.12),五分位数4为1.01(95%可信区间:0.94-1.08),最高收入五分位数(五分位数5)为1.03(95%可信区间:0.96-1.12)。对于1年死亡率,与最低收入五分位数相比,五分位数2的调整比值比为1.01(95%可信区间:0.96-1.06),五分位数3为0.99(95%可信区间:0.94-1.04),五分位数4为0.99(95%可信区间:0.93-1.05),最高收入五分位数为1.03(95%可信区间:0.97-1.10)。
在加拿大安大略省,社会经济地位与社区获得性肺炎老年患者的死亡率无关。