Le Loët Xavier, Pavelka Karel, Richarz Ute
Centre Hospitalier Universitaire de Rouen, Hôpitaux Rouen, Rouen, France.
BMC Musculoskelet Disord. 2005 Jun 15;6:31. doi: 10.1186/1471-2474-6-31.
This study was designed to evaluate the utility of transdermal fentanyl (TDF, Durogesic) for the treatment of pain due to osteoarthritis (OA) of the knee or hip, which was not adequately controlled by non-opioid analgesics or weak opioids. The second part of the trial, investigating TDF in patients with rheumatoid arthritis (RA) is reported separately.
Current analgesia was optimised during a 1-week run-in. Patients then received 28 days treatment with TDF starting at 25 microg/hr, with the option to increase the dose until adequate pain control was achieved. Metoclopramide was taken during the first week and then as needed.
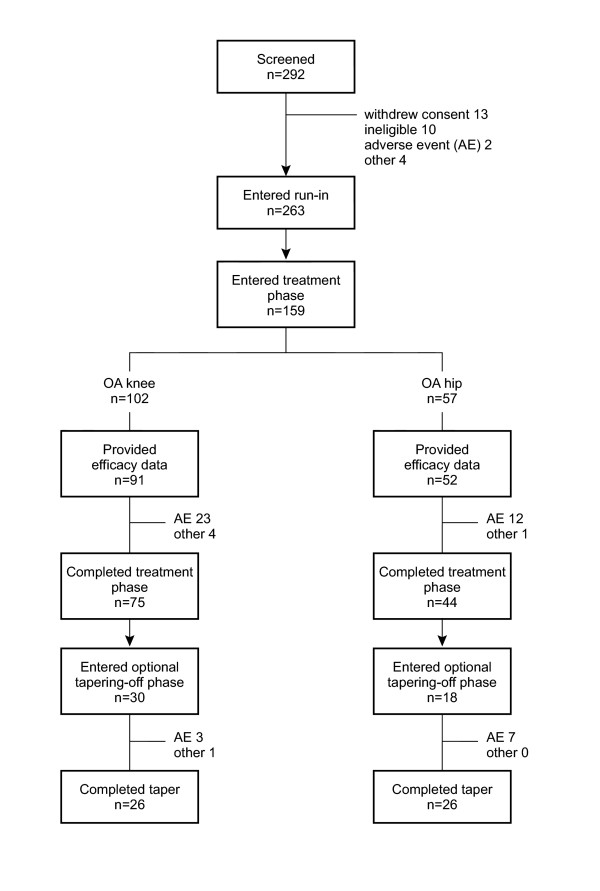
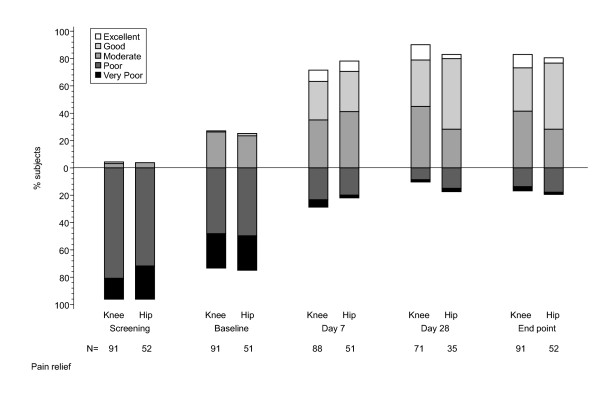
Of the 159 patients recruited, 75 with OA knee and 44 with OA hip completed the treatment phase, 30 knee and 18 hip patients entered the one-week taper-off phase. The most frequently used maximum dose of TDF was 25 microg/hr. The number of patients with adequate pain control increased during the run-in period from 4% to 27%, and further increased during TDF treatment to 88% on day 28. From baseline to endpoint, there were significant reductions in pain (p < 0.001) and improvements in functioning (p < 0.001) and physical (p < 0.001) and mental (p < 0.05) health. Scores for 'pain right now' decreased significantly within 24 hours of starting TDF treatment. TDF was assessed favourably and 84% of patients would recommend it for OA-related pain. Nausea and vomiting were the most common adverse events (reported by 32% and 26% of patients respectively), despite prophylaxis with metoclopramide, which showed limited efficacy in this setting.
TDF significantly increased pain control, and improved functioning and quality of life. Metoclopramide appeared to be of limited value in preventing nausea and vomiting; more effective anti-emetic treatment may enable more people to benefit from strong opioids such as TDF. This study suggests that four weeks is a reasonable period to test the benefit of adding TDF to improve pain control in OA patients and that discontinuing therapy in cases of limited benefit creates no major obstacles.
本研究旨在评估透皮芬太尼(TDF,多瑞吉)用于治疗膝关节或髋关节骨关节炎(OA)所致疼痛的效用,此类疼痛无法通过非阿片类镇痛药或弱阿片类药物得到充分控制。该试验的第二部分,即对类风湿关节炎(RA)患者使用TDF的研究将另行报告。
在为期1周的导入期对当前镇痛方案进行优化。随后患者接受为期28天的TDF治疗,起始剂量为25微克/小时,可选择增加剂量直至疼痛得到充分控制。甲氧氯普胺在第一周服用,之后按需服用。
在招募的159例患者中,75例膝关节OA患者和44例髋关节OA患者完成了治疗阶段,30例膝关节患者和18例髋关节患者进入了为期1周的逐渐减量阶段。TDF最常使用的最大剂量为25微克/小时。在导入期,疼痛得到充分控制的患者数量从4%增至27%,在TDF治疗期间进一步增至第28天时的88%。从基线到终点,疼痛显著减轻(p < 0.001),功能(p < 0.001)、身体(p < 0.001)和精神(p < 0.05)健康状况得到改善。“当下疼痛”评分在开始TDF治疗后24小时内显著降低。TDF得到了良好评价,84%的患者会推荐其用于OA相关疼痛。恶心和呕吐是最常见的不良事件(分别有32%和26%的患者报告),尽管使用了甲氧氯普胺进行预防,但在这种情况下其疗效有限。
TDF显著提高了疼痛控制水平,改善了功能和生活质量。甲氧氯普胺在预防恶心和呕吐方面似乎价值有限;更有效的止吐治疗可能使更多人受益于如TDF这样的强阿片类药物。本研究表明,四周是测试添加TDF改善OA患者疼痛控制效果的合理时长,且在获益有限的情况下停止治疗不会造成重大障碍。