Shah Maulik, Bogucki Brian, Mavers Melissa, deMello Daphne E, Knutsen Alan
Division of Medical Genetics, Department of Pediatrics, Saint Louis University, 1465 South Grand Blvd., Saint Louis, MO 63104-1095, USA.
BMC Med Genet. 2005 Jul 25;6:28. doi: 10.1186/1471-2350-6-28.
Since it's recognition in 1981, a more complete phenotype of Kabuki syndrome is becoming evident as additional cases are identified. Congenital heart defects and a number of visceral abnormalities have been added to the typical dysmorphic features originally described.
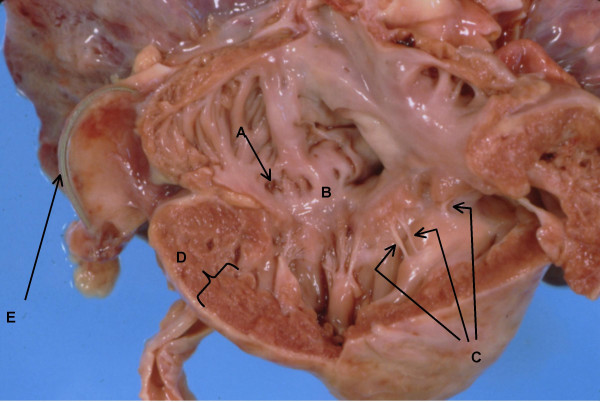
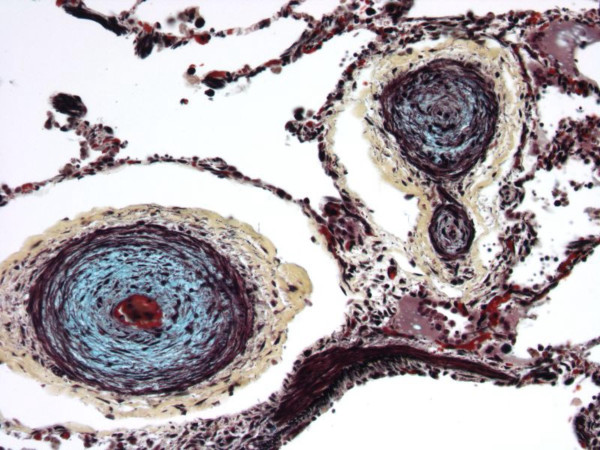
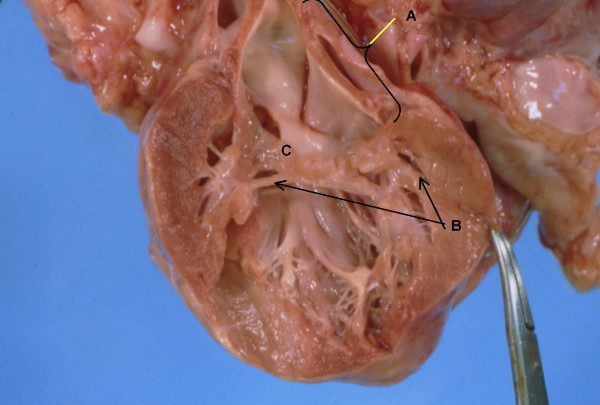
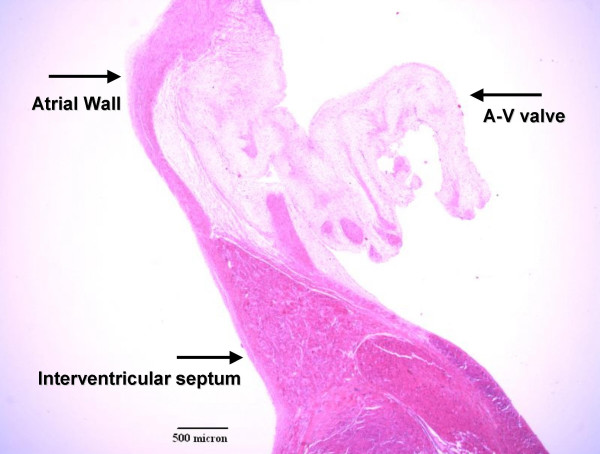
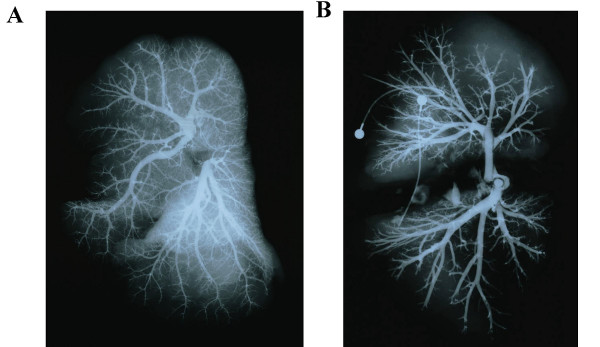
In this report we describe the clinical course of a child diagnosed with Kabuki syndrome based on characteristic clinical, radiological and morphologic features who died of a cardiac arrhythmia at 11-months of age. This infant, however, had abnormal pulmonary architecture and alterations in his cardiac conduction system resulting in episodes of bradycardia and asystole. This child also had an immunological phenotype consistent with common variable immunodeficiency. His clinical course consisted of numerous hospitalizations for recurrent bacterial infections and congenital hypogammaglobulinemia characterized by low serum IgG and IgA but normal IgM levels, and decreased antibody levels to immunizations. T-, B- and NK lymphocyte subpopulations and T-cell function studies were normal.
This child may represent a more severe phenotype of Kabuki syndrome. Recurrent infections in a child should prompt a thorough immunological evaluation. Additionally, electrophysiology testing may be indicated if cardiopulmonary events occur which are not explained by anatomic defects.
自1981年被发现以来,随着更多病例被确诊,歌舞伎综合征更完整的表型正变得愈发明显。先天性心脏缺陷和一些内脏异常已被纳入最初描述的典型畸形特征之中。
在本报告中,我们描述了一名基于特征性临床、放射学和形态学特征被诊断为歌舞伎综合征的儿童的临床病程,该儿童在11个月大时死于心律失常。然而,这名婴儿存在异常的肺部结构以及心脏传导系统改变,导致心动过缓和心搏停止发作。这名儿童还具有与常见变异型免疫缺陷一致的免疫表型。他的临床病程包括因反复细菌感染多次住院,以及先天性低丙种球蛋白血症,其特征为血清IgG和IgA水平低但IgM水平正常,且对免疫接种的抗体水平降低。T细胞、B细胞和NK淋巴细胞亚群以及T细胞功能研究均正常。
这名儿童可能代表歌舞伎综合征更严重的表型。儿童反复感染应促使进行全面的免疫学评估。此外,如果发生无法用解剖缺陷解释的心肺事件,可能需要进行电生理检查。