Jones Daryl, Bates Samantha, Warrillow Stephen, Opdam Helen, Goldsmith Donna, Gutteridge Geoff, Bellomo Rinaldo
Department of Intensive Care, Melbourne University, Austin Hospital, Melbourne, Australia.
Crit Care. 2005 Aug;9(4):R303-6. doi: 10.1186/cc3537. Epub 2005 Apr 28.
Hospital medical emergency teams (METs) have been implemented to reduce cardiac arrests and hospital mortality. The timing and system factors associated with their activation are poorly understood. We sought to determine the circadian pattern of MET activation and to relate it to nursing and medical activities.
We conducted a retrospective observational study of the time of activation for 2568 incidents of MET attendance. Each attendance was allocated to one of 48 half-hour intervals over the 24-hour daily cycle. Activation was related nursing and medical activities.
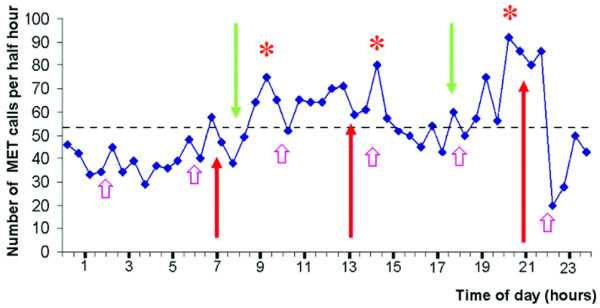
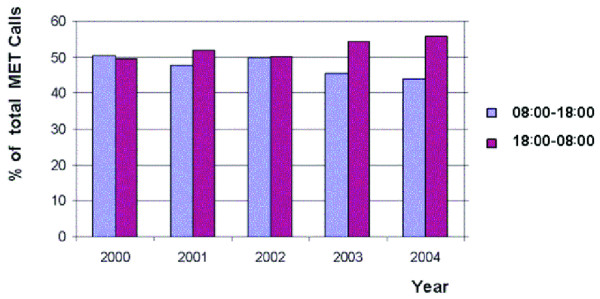
During the study period there were 120,000 consecutive overnight medical and surgical admissions. The hourly rate of MET calls was greater during the day (47% of calls in the 10 hours between 08:00 and 18:00), but 53% of the 2568 calls occurred between 18:00 and 08:00 hours. MET calls increased in the half-hour after routine nursing observation, and in the half-hour before each nursing handover. MET service utilization was 1.25 (95% confidence interval [CI] = 1.11-1.52) times more likely in the three 1-hour periods spanning routine nursing handover (P = 0.001). The greatest level of half-hourly utilization was seen between 20:00 and 20:30 (odds ratio [OR] = 1.76, 95% CI = 1.25-2.48; P = 0.001), before the evening nursing handover. Additional peaks were seen following routine nursing observations between 14:00 and 14:30 (OR = 1.53, 95% CI = 1.07-2.17; P = 0.022) and after the commencement of the daily medical shift (09:00-09:30; OR = 1.43, 95% CI = 1.00-2.04; P = 0.049).
Peak levels of MET service activation occur around the time of routine observations and nursing handover. Our findings raise questions about the appropriate frequency and methods of observation in at-risk hospital patients, reinforce the need for adequately trained medical staff to be available 24 hours per day, and provide useful information for allocation of resources and personnel for a MET service.
医院医疗应急团队(METs)已被设立以减少心脏骤停和医院死亡率。但其启动相关的时间和系统因素仍知之甚少。我们试图确定MET启动的昼夜模式,并将其与护理和医疗活动联系起来。
我们对2568起MET出勤事件的启动时间进行了回顾性观察研究。每次出勤被分配到24小时日常周期中的48个半小时时间段之一。启动与护理和医疗活动相关。
在研究期间,共有120,000例连续的夜间医疗和外科住院病例。白天MET呼叫的每小时发生率更高(08:00至18:00的10小时内占呼叫的47%),但2568次呼叫中有53%发生在18:00至08:00之间。MET呼叫在常规护理观察后的半小时以及每次护理交接班前的半小时增加。在跨越常规护理交接班的三个1小时时间段内,MET服务利用率高出1.25倍(95%置信区间[CI]=1.11 - 1.52)(P = 0.001)。每半小时利用率的最高水平出现在20:00至20:30之间(优势比[OR]=1.76,95% CI = 1.25 - 2.48;P = 0.001),即夜间护理交接班前。在14:00至14:30的常规护理观察后(OR = 1.53,95% CI = 1.07 - 2.17;P = 0.022)以及每日医疗班次开始后(09:00 - 09:30;OR = 1.43,95% CI = 1.00 - 2.04;P = 0.049)还出现了其他峰值。
MET服务启动的高峰水平出现在常规观察和护理交接班前后。我们的研究结果对高危医院患者的适当观察频率和方法提出了疑问,强化了每天24小时都需要有训练有素的医务人员的必要性,并为MET服务的资源和人员分配提供了有用信息。