Innes H, Billingham L, Gaunt C, Steven N, Marshall E
Clatterbridge Centre for Oncology, Bebington, Wirral, Merseyside CH63 4JY, UK.
Br J Cancer. 2005 Dec 12;93(12):1324-8. doi: 10.1038/sj.bjc.6602872.
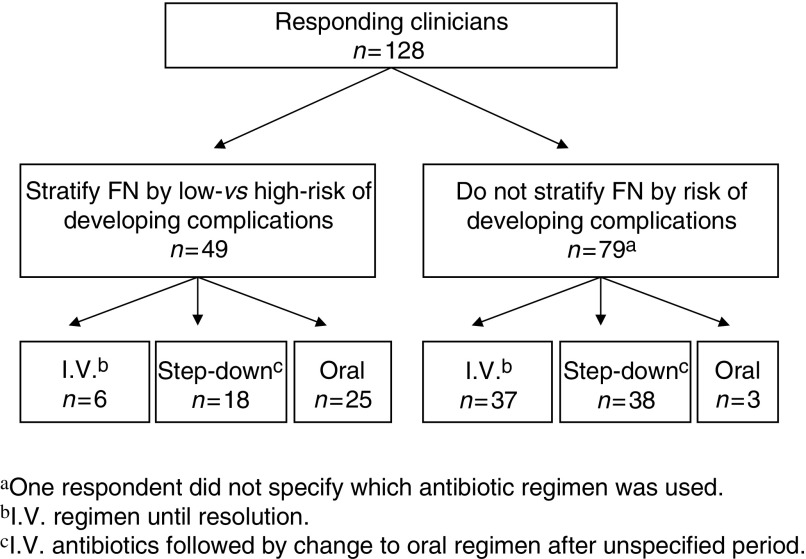
Recent advances in febrile neutropenia (FN) have highlighted the value of risk stratification and the evolving role of oral antibiotics with early hospital discharge in low-risk patients. The aim of this study was to survey whether these advances have been translated into routine clinical practice in the UK. Questionnaires were sent to cancer clinicians across the UK to determine clinicians' routine management of FN, including use of risk stratification, antibiotic regimen and criteria for hospital discharge. In all, 128 clinicians responded, representing 50 cancer departments (83%). Only 38% of respondents stratify patients according to risk and with substantial variation in the criteria defining 'low-risk'. Furthermore, only 22% of clinicians use oral antibiotics as first-line treatment in any patients with FN, but this was significantly greater among clinicians who do compared to those who do not stratify patients by risk, 51 vs 4% (P<0.0001). These findings suggest a slow and/or cautious introduction of newer strategies for the management of low-risk FN in the UK. However, 84% of respondents confirmed their willingness to participate in a trial of oral antibiotics combined with early discharge in low-risk FN.
发热性中性粒细胞减少症(FN)的最新进展凸显了风险分层的价值以及口服抗生素在低风险患者早期出院方面不断演变的作用。本研究的目的是调查这些进展是否已在英国转化为常规临床实践。向英国各地的癌症临床医生发送了问卷,以确定临床医生对FN的常规管理,包括风险分层的使用、抗生素方案和出院标准。共有128名临床医生回复,代表50个癌症科室(83%)。只有38%的受访者根据风险对患者进行分层,且在定义“低风险”的标准方面存在很大差异。此外,只有22%的临床医生在任何FN患者中使用口服抗生素作为一线治疗,但在对患者进行风险分层的临床医生中,这一比例显著高于未进行分层的临床医生,分别为51%和4%(P<0.0001)。这些发现表明,在英国,低风险FN管理的新策略引入缓慢和/或谨慎。然而,84%的受访者确认他们愿意参与一项低风险FN口服抗生素联合早期出院的试验。