Poeze Martijn, Greve Jan Willem M, Ramsay Graham
Department of Surgery, University Hospital Maastricht, P Debyelaan 25, 6202 AZ Maastricht, The Netherlands.
Crit Care. 2005;9(6):R771-9. doi: 10.1186/cc3902. Epub 2005 Nov 15.
To review systematically the effect of interventions aimed at hemodynamic optimization and to relate this to the quality of individual published trials.
A systematic, computerized bibliographic search of published studies and citation reviews of relevant studies was performed. All randomized clinical trials in which adult patients were included in a trial deliberately aiming at an optimized or maximized hemodynamic condition of the patients (with oxygen delivery, cardiac index, oxygen consumption, mixed venous oxygen saturation and/or stroke volume as end-points) were selected. A total of 30 studies were selected for independent review. Two reviewers extracted data on population, intervention, outcome and methodological quality. Agreement between reviewers was high: differences were eventually resolved by third-party decision. The methodological quality of the studies was moderate (mean 9.0, SD 1.7), and the outcomes of the randomized clinical trials were not related to their quality.
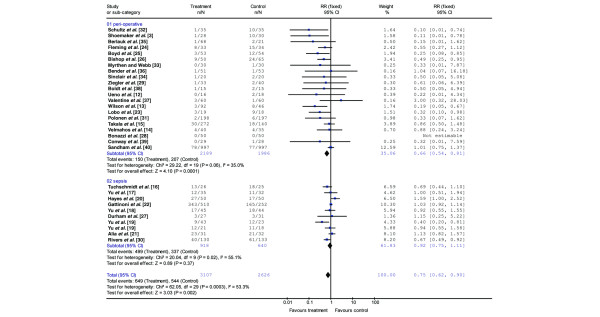
Efforts to achieve an optimized hemodynamic condition resulted in a decreased mortality rate (relative risk ratio (RR) 0.75 (95% confidence interval (CI) 0.62 to 0.90) in all studies combined. This was due to a significantly decreased mortality in peri-operative intervention studies (RR 0.66 (95% CI 0.54 to 0.81). Overall, patients with sepsis and overt organ failure do not benefit from this method (RR 0.92 (95% CI 0.75 to 1.11)).
This systematic review showed that interventions aimed at hemodynamic optimization reduced mortality. In particular, trials including peri-operative interventions aimed at the hemodynamic optimization of high-risk surgical patients reduce mortality. Overall, this effect was not related to the trial quality.
系统回顾旨在实现血流动力学优化的干预措施的效果,并将其与已发表的个体试验的质量相关联。
对已发表的研究进行系统的计算机化文献检索,并对相关研究进行引文综述。选择所有将成年患者纳入旨在优化或最大化患者血流动力学状况(以氧输送、心脏指数、氧消耗、混合静脉血氧饱和度和/或每搏量为终点)的试验的随机临床试验。共选择30项研究进行独立综述。两名评审员提取了关于人群、干预措施、结局和方法学质量的数据。评审员之间的一致性很高:差异最终通过第三方决定解决。研究的方法学质量中等(平均9.0,标准差1.7),随机临床试验的结局与质量无关。
在所有研究中,旨在实现优化血流动力学状况的努力导致死亡率降低(合并相对风险比(RR)为0.75(95%置信区间(CI)为0.62至0.90))。这是由于围手术期干预研究中的死亡率显著降低(RR为0.66(95%CI为0.54至0.81))。总体而言,脓毒症和明显器官衰竭的患者无法从该方法中获益(RR为0.92(95%CI为0.75至1.11))。
该系统评价表明,旨在优化血流动力学的干预措施可降低死亡率。特别是,针对高危手术患者血流动力学优化的围手术期干预试验可降低死亡率。总体而言,这种效果与试验质量无关。