Balamurugan Appathurai, Rivera Mark, Jack Leonard, Allen Kristen, Morris Sharon
Arkansas Department of Health and Human Services, 4815 W Markham, Slot 32, Little Rock, AR 72205, USA.
Prev Chronic Dis. 2006 Jan;3(1):A15. Epub 2005 Dec 15.
Diabetes prevalence has reached epidemic proportions. Diabetes self-management education (DSME) has been shown to improve preventive care practices and clinical outcomes. In this study, we discuss the barriers faced during the implementation of DSME programs in medically underserved rural areas of Arkansas.
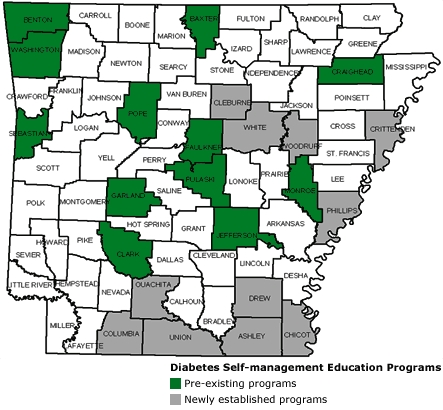
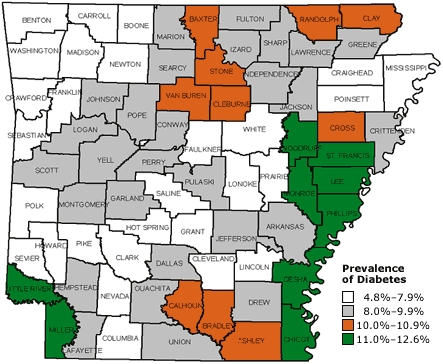
Arkansas is a rural state, with most southeastern counties experiencing a shortage of health care professionals. The Arkansas Diabetes Prevention and Control Program and its partners established 12 DSME programs in underserved counties with a high prevalence of diabetes.
DSME programs were delivered by a registered nurse and a dietitian who provided 10 to 13 hours of education to each program participant. Baseline, 6-month, and year-end data were collected on preventive care practices, such as daily blood glucose monitoring, foot examination, systolic and diastolic blood pressure, and glycosylated hemoglobin level, among the participants in newly established DSME programs.
Of the 12 DSME programs established, 11 received American Diabetes Association recognition. The number of participants in the DSME programs increased 138% in 1 year, from 308 in February 2003 to 734 in March 2004. Preventive care practices improved: daily blood glucose monitoring increased from 56% to 67% of participants, and daily foot examinations increased from 63% to 84% of participants. Glycosylated hemoglobin decreased by an average of 0.5 units per participant who completed the program. However, many anticipated and a few unanticipated barriers during the implementation of the program could not be overcome because of the lack of an evaluation plan.
Although results point to potential benefits of preventive care practices among DSME participants, interpretation of findings was limited by sample size. Sample size limitations are traced to barriers to assessing program outcome. Program evaluation should be integrated into the planning phase to ensure adequate measures of program effectiveness.
糖尿病患病率已达到流行程度。糖尿病自我管理教育(DSME)已被证明可改善预防保健措施和临床结果。在本研究中,我们讨论了在阿肯色州医疗服务不足的农村地区实施DSME项目过程中所面临的障碍。
阿肯色州是一个农村州,东南部的大多数县都面临医疗保健专业人员短缺的问题。阿肯色州糖尿病预防与控制项目及其合作伙伴在糖尿病患病率高且医疗服务不足的县设立了12个DSME项目。
DSME项目由一名注册护士和一名营养师提供,他们为每个项目参与者提供10至13小时的教育。收集了新设立的DSME项目参与者的预防保健措施的基线、6个月和年终数据,如每日血糖监测、足部检查、收缩压和舒张压以及糖化血红蛋白水平。
在设立的12个DSME项目中,11个获得了美国糖尿病协会的认可。DSME项目的参与者人数在1年内增加了138%,从2003年2月的308人增加到2004年3月的734人。预防保健措施得到改善:每日血糖监测的参与者比例从56%增加到67%,每日足部检查的参与者比例从63%增加到84%。完成该项目的参与者糖化血红蛋白平均下降了0.5个单位。然而,由于缺乏评估计划,该项目实施过程中的许多预期障碍和一些意外障碍无法克服。
尽管结果表明DSME参与者的预防保健措施有潜在益处,但研究结果的解读受到样本量的限制。样本量的限制可追溯到评估项目结果的障碍。项目评估应纳入规划阶段,以确保对项目有效性进行充分衡量。