Burton C, Linch D, Hoskin P, Milligan D, Dyer M J S, Hancock B, Mouncey P, Smith P, Qian W, MacLennan K, Jack A, Webb A, Cunningham D
University College London and CRUK Clinical Trials Centre, 222 Euston Road, London NW1 2DA, UK.
Br J Cancer. 2006 Mar 27;94(6):806-13. doi: 10.1038/sj.bjc.6602975.
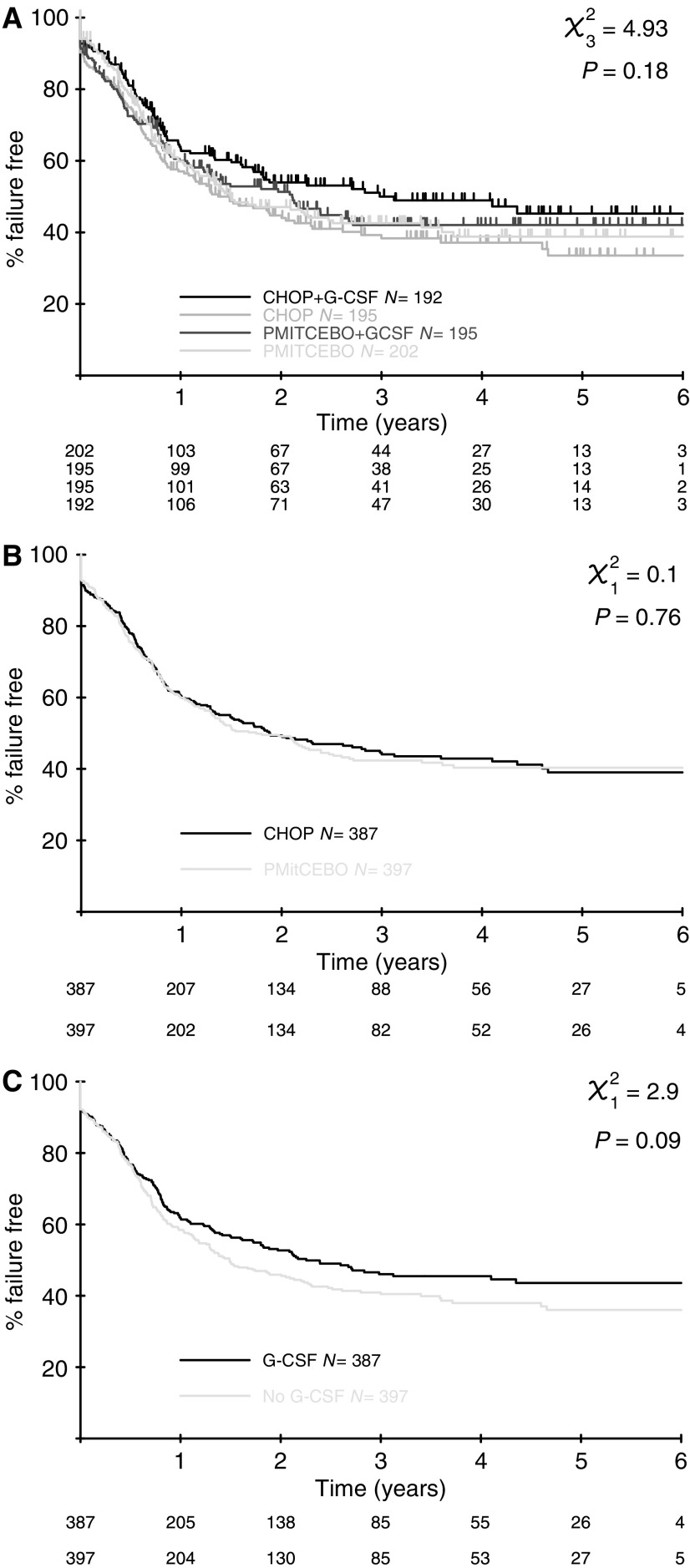
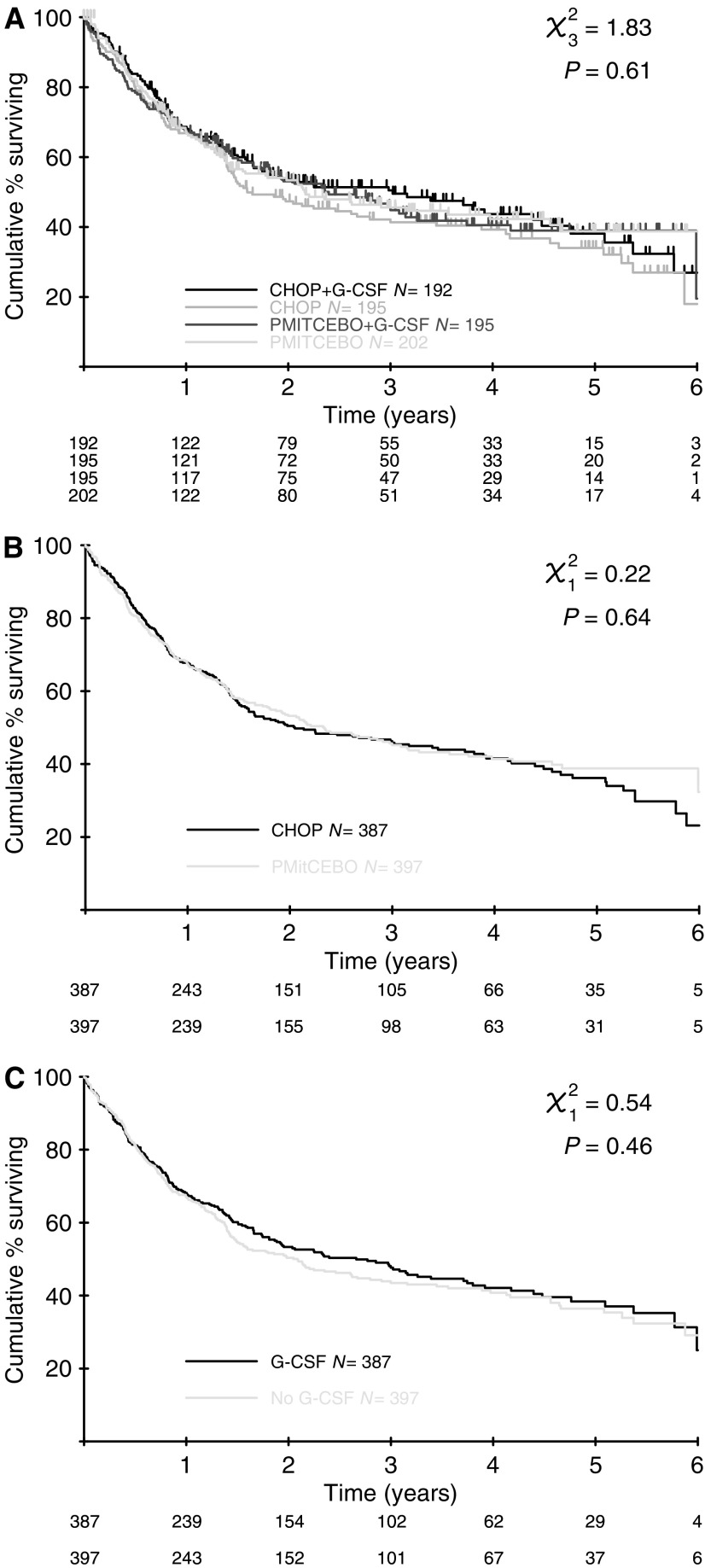
The management of older patients with aggressive non-Hodgkin's lymphoma presents a challenge to the physician. Age is a poor prognostic indicator, due to reduced ability to tolerate and maintain dose-intensive chemotherapy. Generally, older patients demonstrate a lower response rate, reduced survival and increased toxicity, although the majority of large randomised trials exclude older patients. This randomised trial was conducted in patients 60 years or over to compare CHOP (cyclophosphamide 750 mg m(-2), doxorubicin 50 mg m(-2), vincristine 1.4 mg m(-2), prednisolone 100 mg) with PMitCEBO (mitoxantrone 7 mg m(-2), cyclophosphamide 300 mg m(-2), etoposide 150 mg m(-2), vincristine 1.4 mg m(-2), bleomycin 10 mg m(-2) and prednisolone 50 mg). Due to the myelosuppressive nature of these regimens, patients were also randomised to the addition of G-CSF. The formal results of this trial with long-term follow-up are now reported. Data were analysed to assess efficacy and toxicity. Overall response rate was 84% in the CHOP arm and 83% in the PMitCEBO arm, with overall response rates of 83% for the use of G-CSF and 84% for no G-CSF. At median 44 months follow-up, there was no significant difference in failure-free, progression-free or overall survival between the CHOP and PMitCEBO arms. At 3 years, the actuarial failure-free survival was 44% in CHOP recipients and 42% in PMitCEBO recipients and the 3-year actuarial overall survival was 46% and 45% respectively. There was no significant difference in the failure-free, progression-free or overall survival with the addition of G-CSF.
老年侵袭性非霍奇金淋巴瘤患者的管理对医生来说是一项挑战。年龄是一个不良的预后指标,因为耐受和维持剂量密集化疗的能力下降。一般来说,老年患者的缓解率较低、生存率降低且毒性增加,尽管大多数大型随机试验都将老年患者排除在外。这项随机试验针对60岁及以上的患者进行,比较了CHOP方案(环磷酰胺750 mg/m²、多柔比星50 mg/m²、长春新碱1.4 mg/m²、泼尼松龙100 mg)与PMitCEBO方案(米托蒽醌7 mg/m²、环磷酰胺300 mg/m²、依托泊苷150 mg/m²、长春新碱1.4 mg/m²、博来霉素10 mg/m²和泼尼松龙50 mg)。由于这些方案具有骨髓抑制性质,患者还被随机分组以决定是否添加粒细胞集落刺激因子(G-CSF)。现将这项具有长期随访的试验的正式结果报告如下。对数据进行分析以评估疗效和毒性。CHOP组的总缓解率为84%,PMitCEBO组为83%,使用G-CSF的总缓解率为83%,未使用G-CSF的为84%。在中位随访44个月时,CHOP组和PMitCEBO组在无失败生存期、无进展生存期或总生存期方面无显著差异。3年时,CHOP方案接受者的精算无失败生存率为44%,PMitCEBO方案接受者为42%,3年精算总生存率分别为46%和45%。添加G-CSF在无失败生存期、无进展生存期或总生存期方面无显著差异。