Thai Duy M, Kitagawa Yasuyuki, Choong Peter Fm
Department of Orthopaedics and University of Melbourne Department of Surgery, St. Vincent's Hospital Melbourne, Australia.
Division of Surgical Oncology, Peter MacCallum Cancer Institute, Melbourne, Australia.
Int Semin Surg Oncol. 2006 Mar 1;3:5. doi: 10.1186/1477-7800-3-5.
Metastatic disease to the shoulder girdle is a challenging problem because of the potential for pain, pathologic fracture and loss of function of that limb. Management of the bone disease centers around palliation, prevention of further complications and the preservation of residual function. A variety of surgical options exist for managing metastatic disease to the shoulder girdle and our experience with over 90 patients is reported. We focus on a preferred technique of combining rigid intramedullary nailing with cementation.
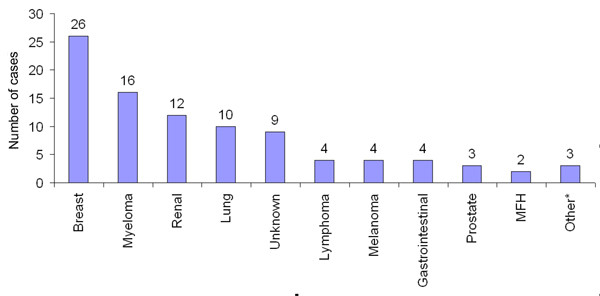
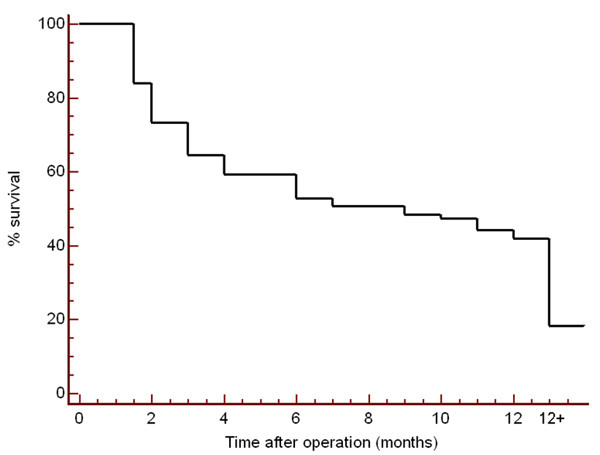
Patients with metastatic disease to the shoulder girdle were accrued over a 9 year period from 1996 to 2004. 93 patients were identified with 96 operations being performed. The median age was 63 years (range 33 - 89) and 54% were female. The commonest primary tumor to metastasize was breast, and the proximal and midshaft humerus was involved in 84% of cases. The median survival time was 8 months and at last review 82% of patients had died of their disease
Operations performed were intramedullary nailing (n = 51), resection with or without prosthetic reconstruction (n = 34) or plate osteosynthesis (n = 9). The site of the metastasis was a guide to the most appropriate operation. Amputations (n = 2) were not done as the primary procedure. Median post operative hospitalization ranged from 3 to 6 days depending on the type of operation performed. Our preferred technique for diaphyseal lesions (intramedullary nailing plus cementation) achieved excellent results in terms of pain relief, functional restoration and minimal complications. Functional restriction was most notable for proximal humeral prostheses (35% of patients).
Surgical treatment of metastases to the shoulder girdle can be successful, allowing prompt relief of pain and return to prehospital level of care. Proximal and midshaft humeral metastases are easily amenable to resection and reconstruction or intramedullary nailing with cementation. Relief of pain and preservation of function occurs for the majority of patients.
肩带转移性疾病是一个具有挑战性的问题,因为存在疼痛、病理性骨折和肢体功能丧失的可能性。骨病的治疗以缓解症状、预防进一步并发症以及保留残余功能为核心。对于肩带转移性疾病,有多种手术选择,本文报告了我们对90余例患者的治疗经验。我们重点介绍一种将刚性髓内钉固定与骨水泥填充相结合的首选技术。
1996年至2004年的9年间,收集了患有肩带转移性疾病的患者。共确定93例患者,实施了96次手术。患者中位年龄为63岁(范围33 - 89岁),女性占54%。最常见的转移原发肿瘤是乳腺癌,84%的病例累及肱骨近端和骨干中段。中位生存时间为8个月,最后一次随访时82%的患者死于疾病。
实施的手术包括髓内钉固定(n = 51)、有或无假体重建的切除术(n = 34)或钢板接骨术(n = 9)。转移部位是选择最合适手术的依据。未将截肢(n = 2)作为主要手术方式。根据所实施的手术类型,术后中位住院时间为3至6天。我们针对骨干病变的首选技术(髓内钉固定加骨水泥填充)在缓解疼痛、功能恢复和并发症最少方面取得了优异效果。肱骨近端假体导致的功能受限最为明显(35%的患者)。
肩带转移性疾病的手术治疗可以成功,能迅速缓解疼痛并恢复到术前护理水平。肱骨近端和骨干中段转移灶易于进行切除和重建或髓内钉固定加骨水泥填充。大多数患者疼痛得到缓解,功能得以保留。