Colton Craig W, Manderscheid Ronald W
Colton & Associates, 475 West 2400 South, Bountiful, UT 84010, USA.
Prev Chronic Dis. 2006 Apr;3(2):A42. Epub 2006 Mar 15.
Mortality rates are used as global measures of a population's health status and as indicators for public health efforts and medical treatments. Elevated mortality rates among individuals with mental illness have been reported in various studies, but very little focus has been placed on interstate comparisons and congruency of mortality and causes of death among public mental health clients.
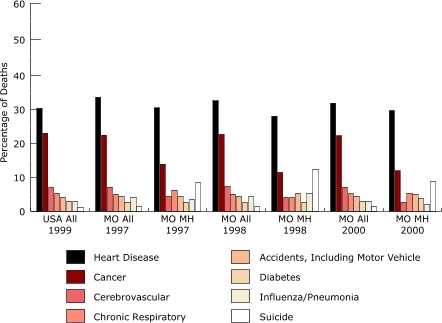
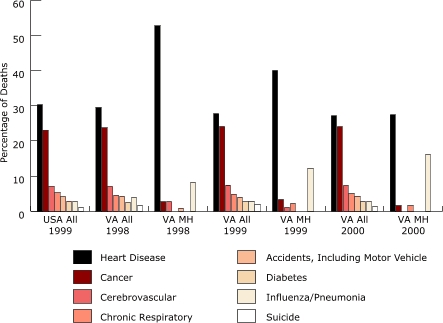
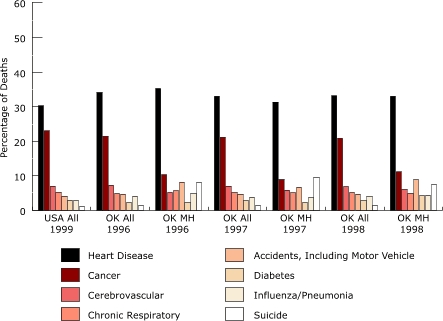
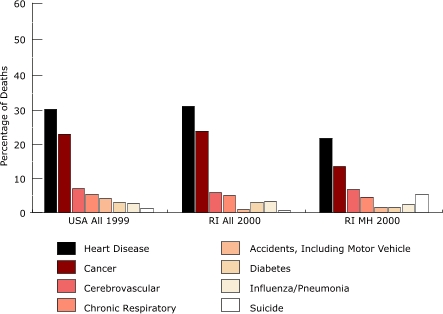
Using age-adjusted death rates, standardized mortality ratios, and years of potential life lost, we compared the mortality of public mental health clients in eight states with the mortality of their state general populations. The data used in our study were submitted by public mental health agencies in eight states (Arizona, Missouri, Oklahoma, Rhode Island, Texas, Utah, Vermont, and Virginia) for 1997 through 2000 during the Sixteen-State Study on Mental Health Performance Measures, a multistate study federally funded by the Center for Mental Health Services in collaboration with the National Association of State Mental Health Program Directors.
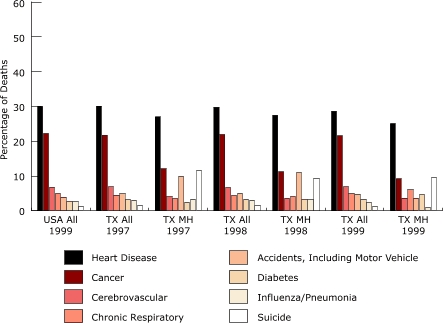
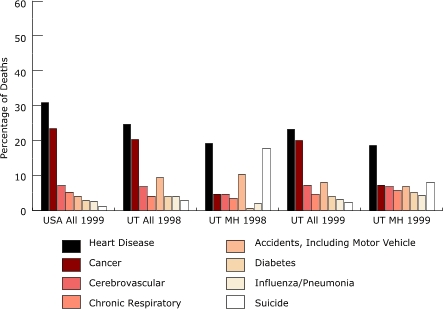
In all eight states, we found that public mental health clients had a higher relative risk of death than the general populations of their states. Deceased public mental health clients had died at much younger ages and lost decades of potential life when compared with their living cohorts nationwide. Clients with major mental illness diagnoses died at younger ages and lost more years of life than people with non-major mental illness diagnoses. Most mental health clients died of natural causes similar to the leading causes of death found nationwide, including heart disease, cancer, and cerebrovascular, respiratory, and lung diseases.
Mental health and physical health are intertwined; both types of care should be provided and linked together within health care delivery systems. Research to track mortality and primary care should be increased to provide information for additional action, treatment modification, diagnosis-specific risk, and evidence-based practices.
死亡率被用作衡量人口健康状况的全球指标,以及公共卫生工作和医疗治疗的指标。各项研究报告了精神疾病患者中较高的死亡率,但很少关注州际比较以及公共心理健康服务对象的死亡率和死因的一致性。
我们使用年龄调整死亡率、标准化死亡比和潜在寿命损失年数,将八个州的公共心理健康服务对象的死亡率与所在州普通人群的死亡率进行了比较。我们研究中使用的数据由八个州(亚利桑那州、密苏里州、俄克拉何马州、罗德岛州、得克萨斯州、犹他州、佛蒙特州和弗吉尼亚州)的公共心理健康机构在1997年至2000年期间提交,这是一项由心理健康服务中心与全国州心理健康项目主任协会合作提供联邦资金的多州研究——十六州心理健康绩效衡量研究。
在所有八个州,我们发现公共心理健康服务对象的死亡相对风险高于所在州的普通人群。与全国范围内的在世同龄人相比,已故的公共心理健康服务对象死亡时年龄要小得多,并且损失了数十年的潜在寿命。患有重度精神疾病诊断的服务对象比患有非重度精神疾病诊断的人死亡时年龄更小,寿命损失更多。大多数心理健康服务对象死于与全国范围内主要死因相似的自然原因,包括心脏病、癌症、脑血管病、呼吸道疾病和肺部疾病。
心理健康与身体健康相互交织;在医疗服务体系中应同时提供并联系这两种类型的护理。应加强跟踪死亡率和初级护理的研究,以提供信息用于进一步的行动、治疗调整、特定诊断风险和循证实践。