Gariballa Salah, Forster Sarah
Sheffield Institute for Nutritional Studies on Ageing, The University of Sheffield, Northern General Hospital, Sheffield, S5 7AU, UK.
Nutr J. 2006 Mar 29;5:9. doi: 10.1186/1475-2891-5-9.
To measure energy expenditure of acutely ill elderly patients in hospital and following discharge in the community.
Sixty-three consecutive hospitalised acutely ill elderly patients were recruited. Eight patients were studied to assess the reliability of the Delta Tract Machine as a measure of energy expenditure; 35 patients had their energy expenditure studied in hospital on two occasions and 20 patients had their energy expenditure measured in hospital and at 6 weeks in the community
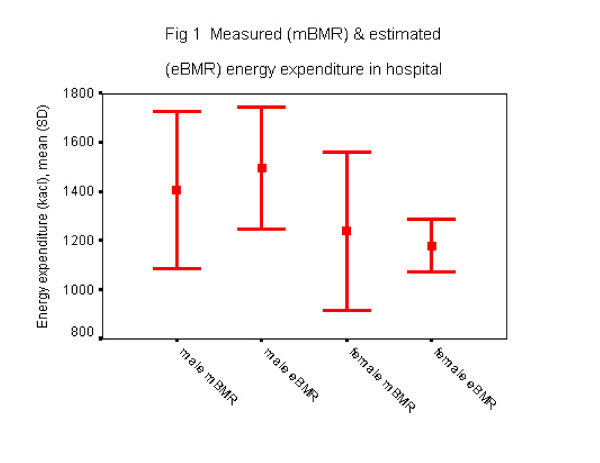
Men had higher basal energy expenditure (BMR) values compared to women however the difference was not statistically significant [Men, mean (SD) 1405 (321) Kcal, women 1238 (322) kcal; mean difference (95% CI) 166 kcal (-17 to 531), p = 0.075]. After adjusting for age, gender and body mass index both medication and C-reactive protein (CRP), concentrations showed significant correlation with measured energy expenditure in hospital, (r = -0.36, "p < 0.05"; r = -0.29, "p < 0.05" respectively). However, in a multivariate analysis for all 63 subjects combined CRP explained most of the variance in BMR in hospital. The Harris Benedict equation predicted within +/- 10% measured BMR in only 47% of individuals in hospital.
Tissue inflammation and medications were associated with change in measured energy expenditure in acutely ill patients.
测量急性病老年患者在住院期间及出院后在社区的能量消耗。
招募了63例连续住院的急性病老年患者。对8例患者进行研究以评估Delta Tract Machine作为能量消耗测量方法的可靠性;35例患者在医院进行了两次能量消耗研究,20例患者在医院及社区6周时测量了能量消耗。
男性的基础能量消耗(BMR)值高于女性,但差异无统计学意义[男性,平均(标准差)1405(321)千卡,女性1238(322)千卡;平均差异(95%可信区间)166千卡(-17至531),p = 0.075]。在调整年龄、性别和体重指数后,药物和C反应蛋白(CRP)浓度均与医院测量的能量消耗显著相关(分别为r = -0.36,“p < 0.05”;r = -0.29,“p < 0.05”)。然而,在对所有63名受试者进行的多变量分析中,CRP解释了医院中BMR的大部分变异。Harris Benedict方程仅在47%的住院患者中预测的BMR与测量值相差±10%以内。
组织炎症和药物与急性病患者测量的能量消耗变化有关。