Oudit Gavin Y, Trivieri Maria G, Khaper Neelam, Liu Peter P, Backx Peter H
Heart and Stroke/Richard Lewar Centre of Excellence, University Health Network, University of Toronto, Ontario, M5S 3E2, Canada.
J Mol Med (Berl). 2006 May;84(5):349-64. doi: 10.1007/s00109-005-0029-x. Epub 2006 Apr 8.
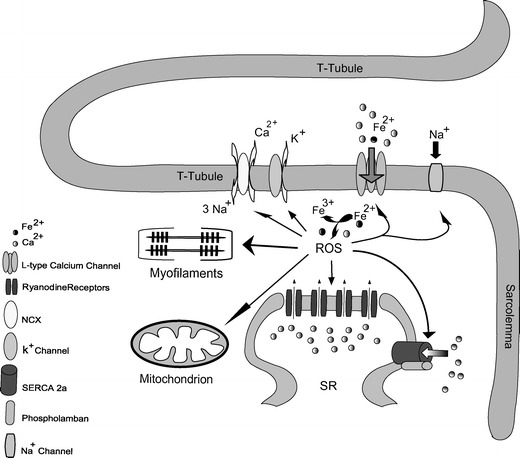
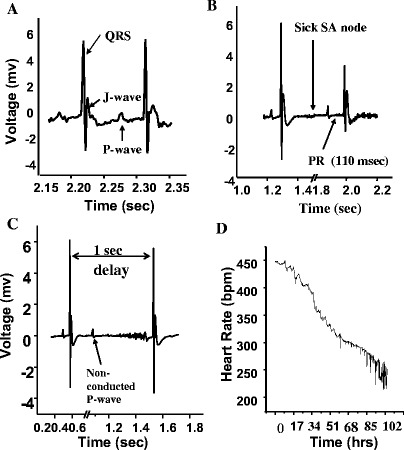
Excessive body iron or iron overload occurs under conditions such as primary (hereditary) hemochromatosis and secondary iron overload (hemosiderosis), which are reaching epidemic levels worldwide. Primary hemochromatosis is the most common genetic disorder with an allele frequency greater than 10% in individuals of European ancestry, while hemosiderosis is less common but associated with a much higher morbidity and mortality. Iron overload leads to iron deposition in many tissues especially the liver, brain, heart and endocrine tissues. Elevated cardiac iron leads to diastolic dysfunction, arrhythmias and dilated cardiomyopathy, and is the primary determinant of survival in patients with secondary iron overload as well as a leading cause of morbidity and mortality in primary hemochromatosis patients. In addition, iron-induced cardiac injury plays a role in acute iron toxicosis (iron poisoning), myocardial ischemia-reperfusion injury, Friedreich ataxia and neurodegenerative diseases. Patients with iron overload also routinely suffer from a range of endocrinopathies, including diabetes mellitus and anterior pituitary dysfunction. Despite clear connections between elevated iron and clinical disease, iron transport remains poorly understood. While low-capacity divalent metal and transferrin-bound transporters are critical under normal physiological conditions, L-type Ca2+ channels (LTCC) are high-capacity pathways of ferrous iron (Fe2+) uptake into cardiomyocytes especially under iron overload conditions. Fe2+ uptake through L-type Ca2+ channels may also be crucial in other excitable cells such as pancreatic beta cells, anterior pituitary cells and neurons. Consequently, LTCC blockers represent a potential new therapy to reduce the toxic effects of excess iron.
体内铁过量或铁过载发生在原发性(遗传性)血色素沉着症和继发性铁过载(含铁血黄素沉着症)等情况下,这些情况在全球正达到流行程度。原发性血色素沉着症是最常见的遗传性疾病,在欧洲血统个体中的等位基因频率大于10%,而含铁血黄素沉着症则较少见,但发病率和死亡率要高得多。铁过载会导致铁在许多组织尤其是肝脏、大脑、心脏和内分泌组织中沉积。心脏铁含量升高会导致舒张功能障碍、心律失常和扩张型心肌病,是继发性铁过载患者生存的主要决定因素,也是原发性血色素沉着症患者发病和死亡的主要原因。此外,铁诱导的心脏损伤在急性铁中毒(铁中毒)、心肌缺血再灌注损伤、弗里德赖希共济失调和神经退行性疾病中起作用。铁过载患者通常还患有一系列内分泌疾病,包括糖尿病和垂体前叶功能障碍。尽管铁含量升高与临床疾病之间的联系很明显,但铁的转运仍知之甚少。虽然低容量二价金属和转铁蛋白结合转运体在正常生理条件下至关重要,但L型钙通道(LTCC)是亚铁(Fe2+)进入心肌细胞的高容量途径,尤其是在铁过载情况下。通过L型钙通道摄取Fe2+在其他可兴奋细胞如胰腺β细胞、垂体前叶细胞和神经元中可能也很关键。因此,LTCC阻滞剂代表了一种潜在的新疗法,可减少过量铁的毒性作用。