Park Joo Hun, Koh Younsuck, Lim Chae-Man, Hong Sang-Bum, Oh Yeon Mok, Shim Tae Sun, Lee Sang Do, Kim Woo Sung, Kim Dong Soon, Kim Won Dong
Department of Pulmonary and Critical Care Medicine, Ajou University School of Medicine, Suwon, Korea.
Korean J Intern Med. 2006 Mar;21(1):1-9. doi: 10.3904/kjim.2006.21.1.1.
There are contradictory reports concerning hypercapnia as a predictor of a better outcome in COPD. This study examined the clinical implications of hypercapnea in COPD patients (M:F = 59:19) who required mechanical ventilation.
The clinical parameters at the time of MICU admission, the total ventilation time, the APACHE II score and the pulmonary function testing were retrospectively analyzed between the survivors and nonsurvivors.
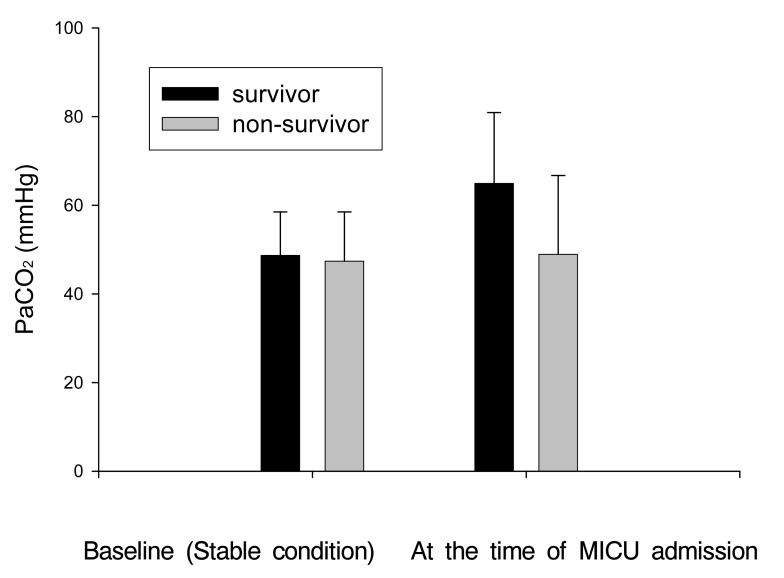
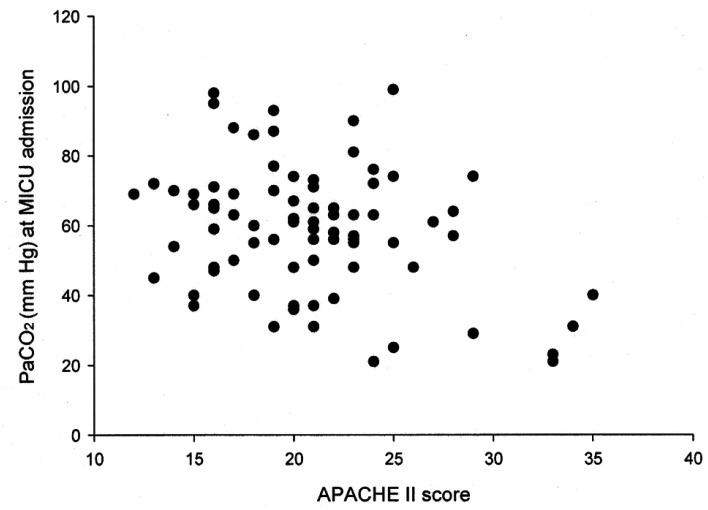
Univariate analysis showed that compared with the nonsurvivors, the survivors had lower AaDO2 values (59.8 +/- 53.5 vs. 105.0 +/- 73.3 mmHg, p=0.000), higher PaCO2 values (64.9 +/- 16.0 vs. 48.9 +/- 17.8 mmHg, p=0.000), lower APACHE II scores (19.0 +/- 3.8 vs. 24.1 +/- 5.1, p=0.002), the more frequent application of initial noninvasive positive pressure ventilation (44.0 vs. 14.3%, p=0.008), and a lower combined rate of septic shock (4.0 vs. 39.3%, p=0.000). Multivariate analysis revealed that a lower PaCO2 (OR: 0.94, p=0.008), the presence of septic shock (OR: 10.16, p=0.011), a higher APACHE II score (OR: 1.22, p=0.040) and a longer ventilation time (OR: 1.002, p=0.041) were the risk factors for mortality. A lower PaCO2 was also verified as the predictor. for mortality by multivariate analysis when excluding septic shock.
Hypercapnia at admission is thought to be an independent predictor of better survival for the COPD patients who require mechanical ventilation.
关于高碳酸血症作为慢性阻塞性肺疾病(COPD)预后较好的预测指标,存在相互矛盾的报道。本研究探讨了需要机械通气的COPD患者(男:女 = 59:19)中高碳酸血症的临床意义。
回顾性分析了幸存者和非幸存者入住重症监护病房(MICU)时的临床参数、总通气时间、急性生理与慢性健康状况评分系统(APACHE II)评分及肺功能测试结果。
单因素分析显示,与非幸存者相比,幸存者的肺泡 - 动脉血氧分压差(AaDO2)值较低(59.8±53.5 vs. 105.0±73.3 mmHg,p = 0.000),动脉血二氧化碳分压(PaCO2)值较高(64.9±16.0 vs. 48.9±17.8 mmHg,p = 0.000),APACHE II评分较低(19.0±3.8 vs. 24.1±5.1,p = 0.002),初始无创正压通气的应用更为频繁(44.0% vs. 14.3%,p = 0.008),脓毒性休克的合并发生率较低(4.0% vs. 39.3%,p = 0.000)。多因素分析显示,较低的PaCO2(比值比[OR]:0.94, p = 0.008)、脓毒性休克的存在(OR:10.16, p = 0.011)、较高的APACHE II评分(OR:1.22, p = 0.040)和较长的通气时间(OR:1.002, p = 0.041)是死亡的危险因素。排除脓毒性休克后,多因素分析也证实较低的PaCO2是死亡的预测指标。
入院时的高碳酸血症被认为是需要机械通气的COPD患者生存较好的独立预测指标。