López Sastre José B, Pérez Solís David, Roqués Serradilla Vicente, Fernández Colomer Belén, Coto Cotallo Gil D, Krauel Vidal Xavier, Narbona López Eduardo, García del Río Manuel, Sánchez Luna Manuel, Belaustegui Cueto Antonio, Moro Serrano Manuel, Urbón Artero Alfonso, Alvaro Iglesias Emilio, Cotero Lavín Angel, Martínez Vilalta Eduardo, Jiménez Cobos Bartolomé
Service of Neonatology, Hospital Universitario Central de Asturias, Oviedo, Spain.
BMC Pediatr. 2006 May 18;6:16. doi: 10.1186/1471-2431-6-16.
It has recently been suggested that serum procalcitonin (PCT) is of value in the diagnosis of neonatal sepsis, with varying results. The aim of this prospective multicenter study was to assess the usefulness of PCT as a marker of neonatal sepsis of nosocomial origin.
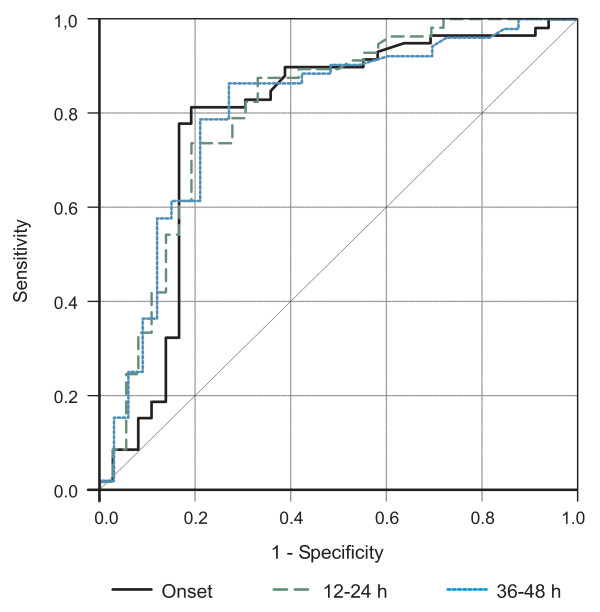
One hundred infants aged between 4 and 28 days of life admitted to the Neonatology Services of 13 acute-care teaching hospitals in Spain over 1-year with clinical suspicion of neonatal sepsis of nosocomial origin were included in the study. Serum PCT concentrations were determined by a specific immunoluminometric assay. The reliability of PCT for the diagnosis of nosocomial neonatal sepsis at the time of suspicion of infection and at 12-24 h and 36-48 h after the onset of symptoms was calculated by receiver-operating characteristics (ROC) curves. The Youden's index (sensitivity + specificity - 1) was used for determination of optimal cutoff values of the diagnostic tests in the different postnatal periods. Sensitivity, specificity, and the likelihood ratio of a positive and negative result with the 95% confidence interval (CI) were calculated.
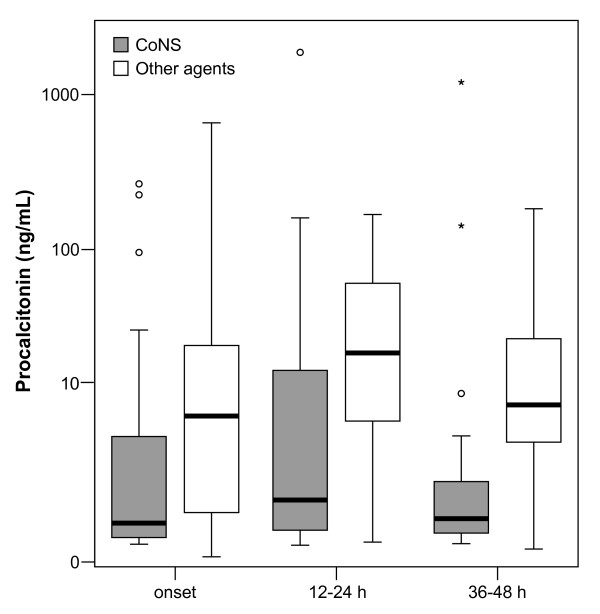
The diagnosis of nosocomial sepsis was confirmed in 61 neonates. Serum PCT concentrations were significantly higher at initial suspicion and at 12-24 h and 36-48 h after the onset of symptoms in neonates with confirmed sepsis than in neonates with clinically suspected but not confirmed sepsis. Optimal PCT thresholds according to ROC curves were 0.59 ng/mL at the time of suspicion of sepsis (sensitivity 81.4%, specificity 80.6%); 1.34 ng/mL within 12-24 h of birth (sensitivity 73.7%, specificity 80.6%), and 0.69 ng/mL within 36-48 h of birth (sensitivity 86.5%, specificity 72.7%).
Serum PCT concentrations showed a moderate diagnostic reliability for the detection of nosocomial neonatal sepsis from the time of suspicion of infection. PCT is not sufficiently reliable to be the sole marker of sepsis, but would be useful as part of a full sepsis evaluation.
最近有人提出,血清降钙素原(PCT)在新生儿败血症的诊断中具有一定价值,但结果不一。这项前瞻性多中心研究的目的是评估PCT作为医院源性新生儿败血症标志物的实用性。
在1年的时间里,纳入了西班牙13家急症护理教学医院新生儿科收治的100名年龄在4至28天之间、临床怀疑为医院源性新生儿败血症的婴儿。通过特定的免疫发光测定法测定血清PCT浓度。通过受试者操作特征(ROC)曲线计算在怀疑感染时以及症状出现后12 - 24小时和36 - 48小时PCT对医院源性新生儿败血症诊断的可靠性。约登指数(敏感度 + 特异度 - 1)用于确定不同产后时期诊断试验的最佳临界值。计算敏感度、特异度以及阳性和阴性结果的似然比及95%置信区间(CI)。
61名新生儿被确诊为医院感染败血症。确诊败血症的新生儿在最初怀疑时以及症状出现后12 - 24小时和36 - 48小时的血清PCT浓度显著高于临床怀疑但未确诊败血症的新生儿。根据ROC曲线,怀疑败血症时的最佳PCT阈值为0.59 ng/mL(敏感度81.4%,特异度80.6%);出生后12 - 24小时内为1.34 ng/mL(敏感度73.7%,特异度80.6%),出生后36 - 48小时内为0.69 ng/mL(敏感度86.5%,特异度72.7%)。
从怀疑感染时起,血清PCT浓度对医院源性新生儿败血症的检测显示出中等的诊断可靠性。PCT作为败血症的唯一标志物不够可靠,但作为全面败血症评估的一部分将是有用的。