Willison Donald J, Kapral Moira K, Peladeau Pierrot, Richards Janice A, Fang Jiming, Silver Frank L
Centre for Evaluation of Medicines, St, Joseph's Healthcare, Department of Clinical Epidemiology & Biostatistics, McMaster University Hamilton, Ontario, Canada.
BMC Med Ethics. 2006 May 23;7:E6. doi: 10.1186/1472-6939-7-6.
In earlier work, we found important selection biases when we tried to obtain consent for participation in a national stroke registry. Recognizing that not all registries will be exempt from requiring consent for participation, we examine here in greater depth the reasons for the poor accrual of patients from a systems perspective with a view to obtaining as representative sample as possible.
We determined the percent of eligible patients who were approached to participate and, among those approached, the percent who actually consented to participate. In addition we examined the reasons why people were not approached or did not consent and the variation across sites in the percent of patients approached and consented. We also considered site variation in restrictions on the accrual and data collection process imposed by either the local research ethics board or the hospital.
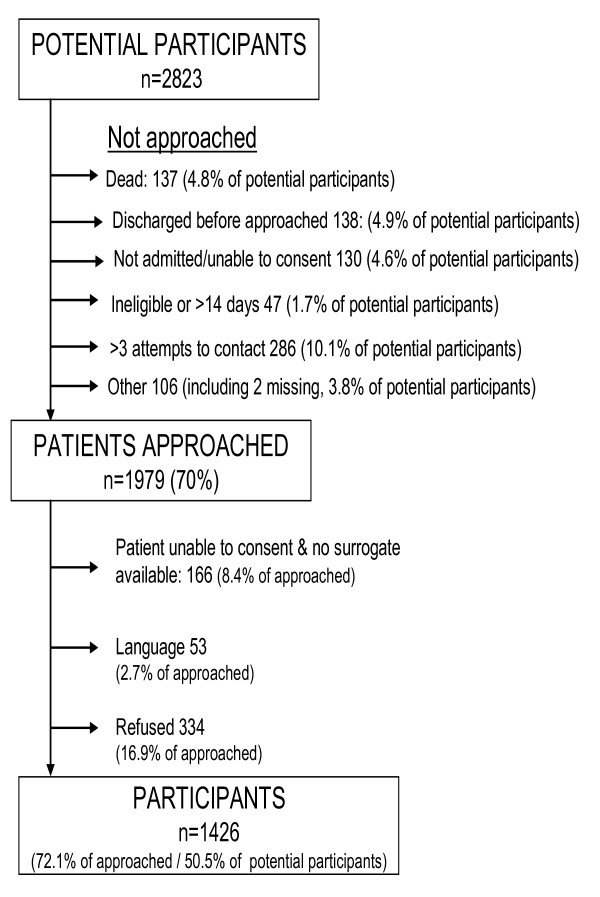
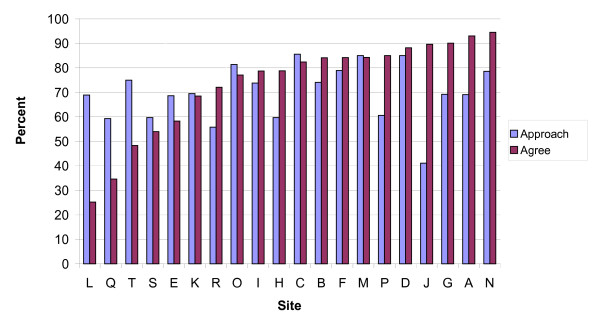
Seventy percent of stroke patients were approached, with wide variations in approach rates across sites (from: 41% to 86%), and considerable inter-site variation in hospital policies governing patient accrual. Chief reasons for not approaching were discharge or death before being approached for consent. Seventeen percent of those approached refused to participate (range: 5% to 75%). Finally, 11% of those approached did not participate due to language or communication difficulties.
We found wide variation in approach and agree rates across sites that were accounted for, in part, by different approaches to accrual and idiosyncratic policies of the hospitals. This wide variation in approach and agree rates raises important challenges for research ethics boards and data protection authorities in determining when to waive consent requirements, when to press for increased quality control, when to permit local adaptation of the consent process, and when to permit alternatives to individual express consent. We offer several suggestions for those registries that require consent for participation.
在早期的研究中,我们发现,在试图获取参与一项全国性卒中登记研究的同意书时,存在重大的选择偏倚。鉴于并非所有登记研究都可免于要求参与者提供同意书,我们从系统角度更深入地研究了患者纳入率低的原因,以期获得尽可能具有代表性的样本。
我们确定了被邀请参与的符合条件患者的百分比,以及在被邀请者中实际同意参与的百分比。此外,我们研究了人们未被邀请或未同意参与的原因,以及各研究点在被邀请和同意参与的患者百分比方面的差异。我们还考虑了当地研究伦理委员会或医院对纳入和数据收集过程所施加限制方面的研究点差异。
70%的卒中患者被邀请参与,各研究点的邀请率差异很大(范围为41%至86%),且各医院在患者纳入政策方面存在显著的研究点间差异。未被邀请的主要原因是在被邀请同意参与之前已出院或死亡。17%的被邀请者拒绝参与(范围为5%至75%)。最后,11%的被邀请者因语言或沟通困难而未参与。
我们发现各研究点在邀请率和同意率方面存在很大差异,部分原因在于不同的纳入方法和医院的特殊政策。这种邀请率和同意率的广泛差异给研究伦理委员会和数据保护机构带来了重大挑战,涉及确定何时可免除同意要求、何时应加强质量控制、何时允许对同意过程进行局部调整,以及何时允许替代个人明确同意的方式。我们为那些需要参与者提供同意书的登记研究提出了若干建议。