Radiation Oncology Branch, Center for Cancer Research, National Cancer Institute, NIH, DHHS, Bldg 10, CRC Rm B2(SW) 3500, 9000 Rockville Pike, Bethesda, MD, 20892, USA.
Radiat Oncol. 2006 Feb 28;1:2. doi: 10.1186/1748-717X-1-2.
We sought to determine the intra- and inter-radiation therapist reproducibility of a previously established matching technique for daily verification and correction of isocenter position relative to intraprostatic fiducial markers (FM).
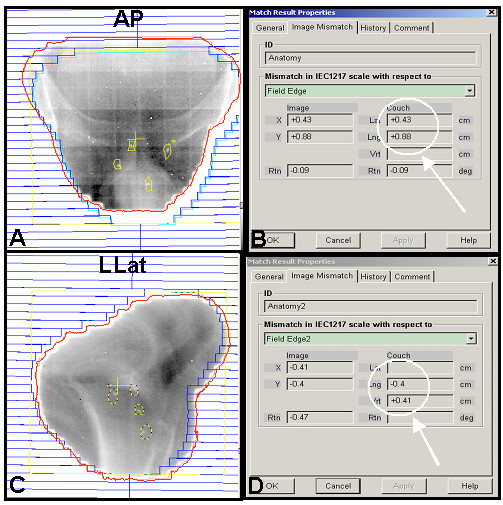
With the patient in the treatment position, anterior-posterior and left lateral electronic images are acquired on an amorphous silicon flat panel electronic portal imaging device. After each portal image is acquired, the therapist manually translates and aligns the fiducial markers in the image to the marker contours on the digitally reconstructed radiograph. The distances between the planned and actual isocenter location is displayed. In order to determine the reproducibility of this technique, four therapists repeated and recorded this operation two separate times on 20 previously acquired portal image datasets from two patients. The data were analyzed to obtain the mean variability in the distances measured between and within observers.
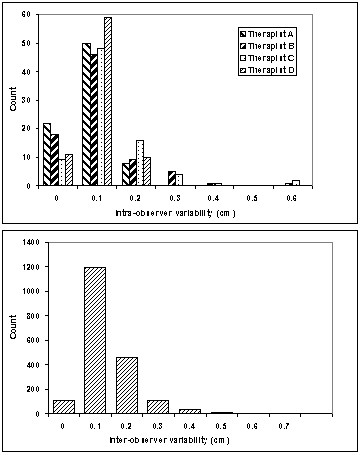
The mean and median intra-observer variability ranged from 0.4 to 0.7 mm and 0.3 to 0.6 mm respectively with a standard deviation of 0.4 to 1.0 mm. Inter-observer results were similar with a mean variability of 0.9 mm, a median of 0.6 mm, and a standard deviation of 0.7 mm. When using a 5 mm threshold, only 0.5% of treatments will undergo a table shift due to intra or inter-observer error, increasing to an error rate of 2.4% if this threshold were reduced to 3 mm.
We have found high reproducibility with a previously established method for daily verification and correction of isocenter position relative to prostatic fiducial markers using electronic portal imaging.
我们旨在确定先前建立的一种匹配技术在每天验证和校正前列腺内基准标记物(FM)相对于等中心位置的内和间放射治疗师可重复性。
在患者处于治疗位置时,使用非晶硅平板电子射野影像装置获取前后和左侧电子图像。获取每个电子射野图像后,治疗师手动将图像中的基准标记物平移并与数字重建射线照片上的标记轮廓对齐。显示计划和实际等中心位置之间的距离。为了确定该技术的可重复性,四名治疗师在两名患者的 20 个先前获取的电子射野图像数据集上两次重复并记录此操作。对数据进行分析以获得观察者之间和内部测量距离的平均可变性。
观察者内的平均和中位数变异性分别为 0.4 至 0.7 毫米和 0.3 至 0.6 毫米,标准偏差为 0.4 至 1.0 毫米。观察者间的结果相似,平均变异性为 0.9 毫米,中位数为 0.6 毫米,标准偏差为 0.7 毫米。当使用 5 毫米的阈值时,只有 0.5%的治疗会由于内或间观察者误差而导致工作台移位,如果将此阈值降低到 3 毫米,则误差率将增加到 2.4%。
我们使用电子射野影像已经发现了一种先前建立的方法,该方法可高度重现性地每天验证和校正前列腺内基准标记物相对于等中心位置。