Wilkins Brad W, Schrage William G, Liu Zhong, Hancock Kellie C, Joyner Michael J
Department of Anesthesiology, Mayo Clinic, Rochester, MN 55905, USA.
J Appl Physiol (1985). 2006 Nov;101(5):1343-50. doi: 10.1152/japplphysiol.00487.2006. Epub 2006 Jun 29.
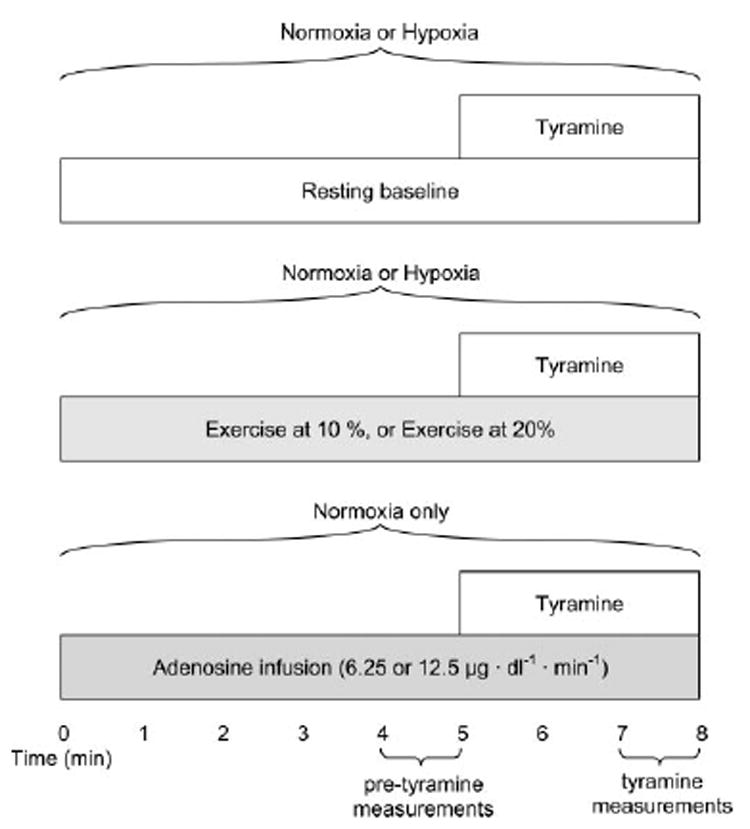
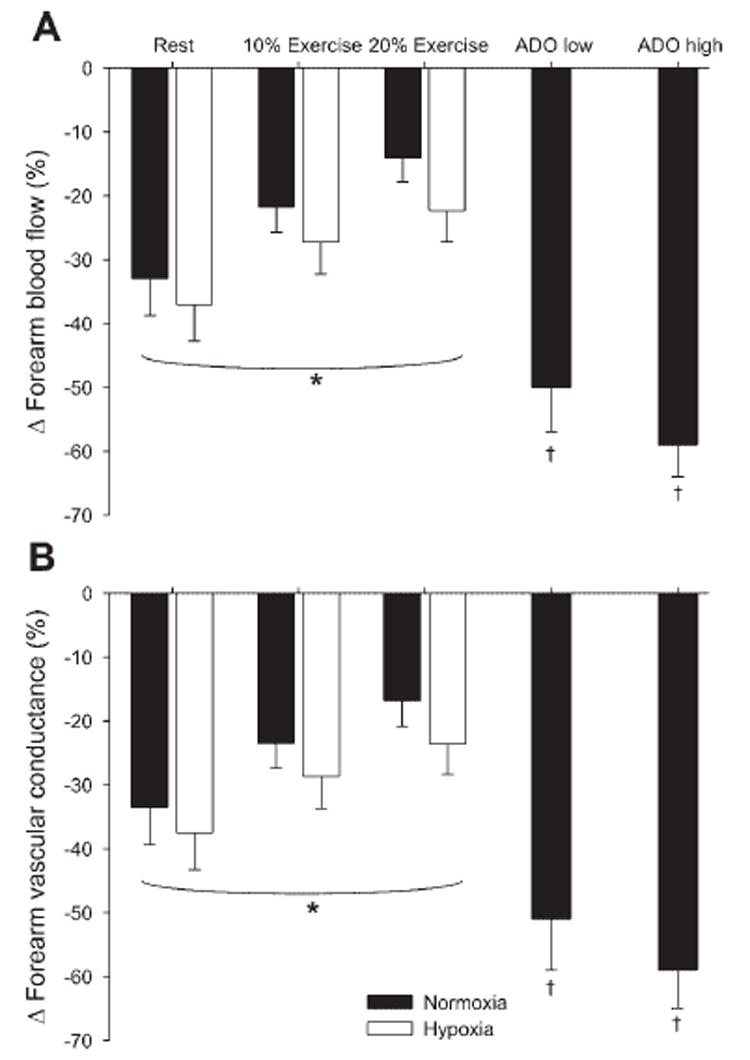
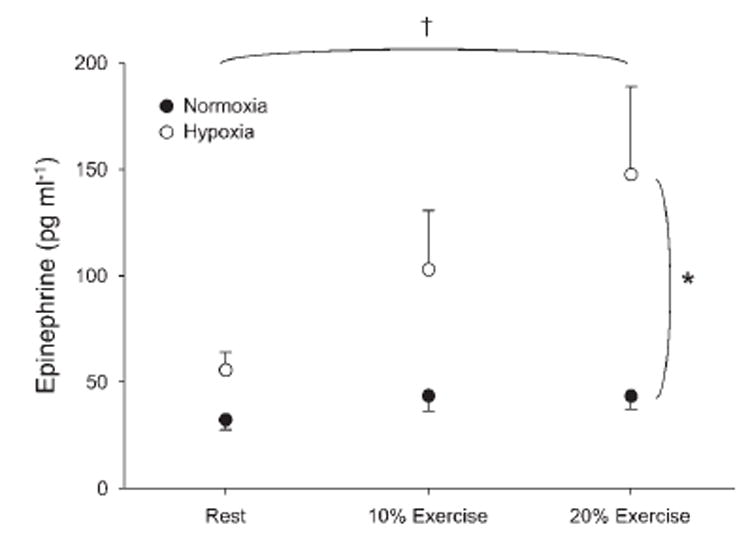
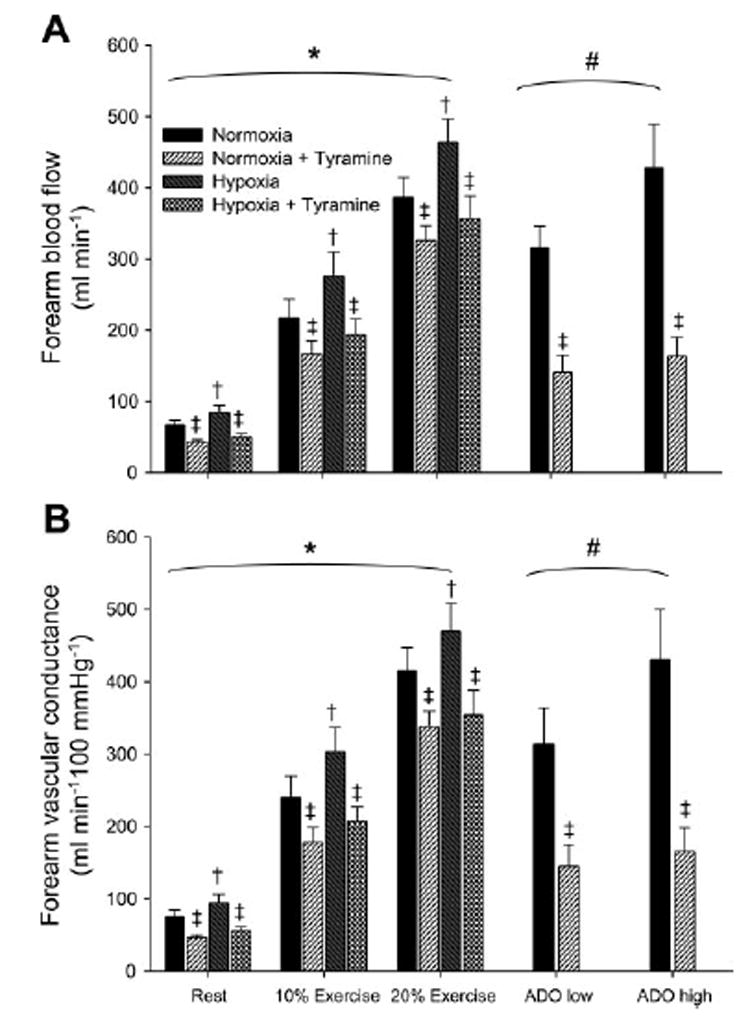
Exercise blunts sympathetic alpha-adrenergic vasoconstriction (functional sympatholysis). We hypothesized that sympatholysis would be augmented during hypoxic exercise compared with exercise alone. Fourteen subjects were monitored with ECG and pulse oximetry. Brachial artery and antecubital vein catheters were placed in the nondominant (exercising) arm. Subjects breathed hypoxic gas to titrate arterial O2 saturation to 80% while remaining normocapnic via a rebreath system. Baseline and two 8-min bouts of rhythmic forearm exercise (10 and 20% of maximum) were performed during normoxia and hypoxia. Forearm blood flow, blood pressure, heart rate, minute ventilation, and end-tidal CO2 were measured at rest and during exercise. Vasoconstrictor responsiveness was determined by responses to intra-arterial tyramine during the final 3 min of rest and each exercise bout. Heart rate was higher during hypoxia (P < 0.01), whereas blood pressure was similar (P = 0.84). Hypoxic exercise potentiated minute ventilation compared with normoxic exercise (P < 0.01). Forearm blood flow was higher during hypoxia compared with normoxia at rest (85 +/- 9 vs. 66 +/- 7 ml/min), at 10% exercise (276 +/- 33 vs. 217 +/- 27 ml/min), and at 20% exercise (464 +/- 32 vs. 386 +/- 28 ml/min; P < 0.01). Arterial epinephrine was higher during hypoxia (P < 0.01); however, venoarterial norepinephrine difference was similar between hypoxia and normoxia before (P = 0.47) and during tyramine administration (P = 0.14). Vasoconstriction to tyramine (%decrease from pretyramine values) was blunted in a dose-dependent manner with increasing exercise intensity (P < 0.01). Interestingly, vasoconstrictor responsiveness tended to be greater (P = 0.06) at rest (-37 +/- 6% vs. -33 +/- 6%), at 10% exercise (-27 +/- 5 vs. -22 +/- 4%), and at 20% exercise (-22 +/- 5 vs. -14 +/- 4%) between hypoxia and normoxia, respectively. Thus sympatholysis is not augmented by moderate hypoxia nor does it contribute to the increased blood flow during hypoxic exercise.
运动可减弱交感α-肾上腺素能血管收缩(功能性交感神经抑制)。我们假设与单纯运动相比,低氧运动期间交感神经抑制会增强。对14名受试者进行心电图和脉搏血氧饱和度监测。在非优势(运动)手臂放置肱动脉和肘前静脉导管。受试者通过再呼吸系统吸入低氧气体,将动脉血氧饱和度滴定至80%,同时保持正常碳酸血症。在常氧和低氧状态下进行基线测量以及两轮8分钟的有节奏前臂运动(最大运动强度的10%和20%)。在休息和运动期间测量前臂血流量、血压、心率、分钟通气量和呼气末二氧化碳。在休息的最后3分钟以及每次运动回合期间,通过对动脉内给予酪胺的反应来确定血管收缩反应性。低氧期间心率较高(P<0.01),而血压相似(P = 0.84)。与常氧运动相比,低氧运动增强了分钟通气量(P<0.01)。在休息时(85±9 vs. 66±7 ml/min)、10%运动强度时(276±33 vs. 217±27 ml/min)和20%运动强度时(464±32 vs. 386±28 ml/min;P<0.01),低氧状态下的前臂血流量均高于常氧状态。低氧期间动脉肾上腺素水平较高(P<0.01);然而,在给予酪胺之前(P = 0.47)以及给予酪胺期间(P = 0.14),低氧和常氧状态下静脉-动脉去甲肾上腺素差值相似。随着运动强度增加,对酪胺的血管收缩反应(相对于酪胺给药前值的降低百分比)呈剂量依赖性减弱(P<0.01)。有趣的是,在休息时(-37±6% vs.-33±6%)、10%运动强度时(-27±5 vs.-22±4%)和20%运动强度时(-22±5 vs.-14±4%),低氧和常氧状态下血管收缩反应性分别倾向于更高(P = 0.06)。因此,中度低氧并不会增强交感神经抑制,也不会导致低氧运动期间血流量增加。