Kötz B S, Croft S, Ferry D R
Division of Cancer Studies, University of Birmingham, Birmingham B15 2TT, and The Royal Wolverhampton Hospital NHS Trust, UK.
Br J Cancer. 2006 Oct 9;95(7):835-40. doi: 10.1038/sj.bjc.6603333. Epub 2006 Sep 12.
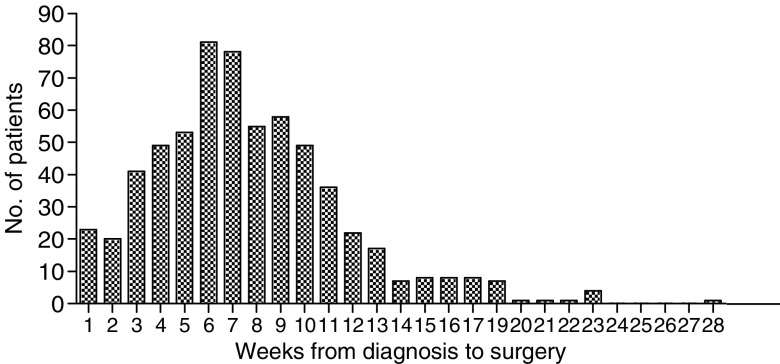
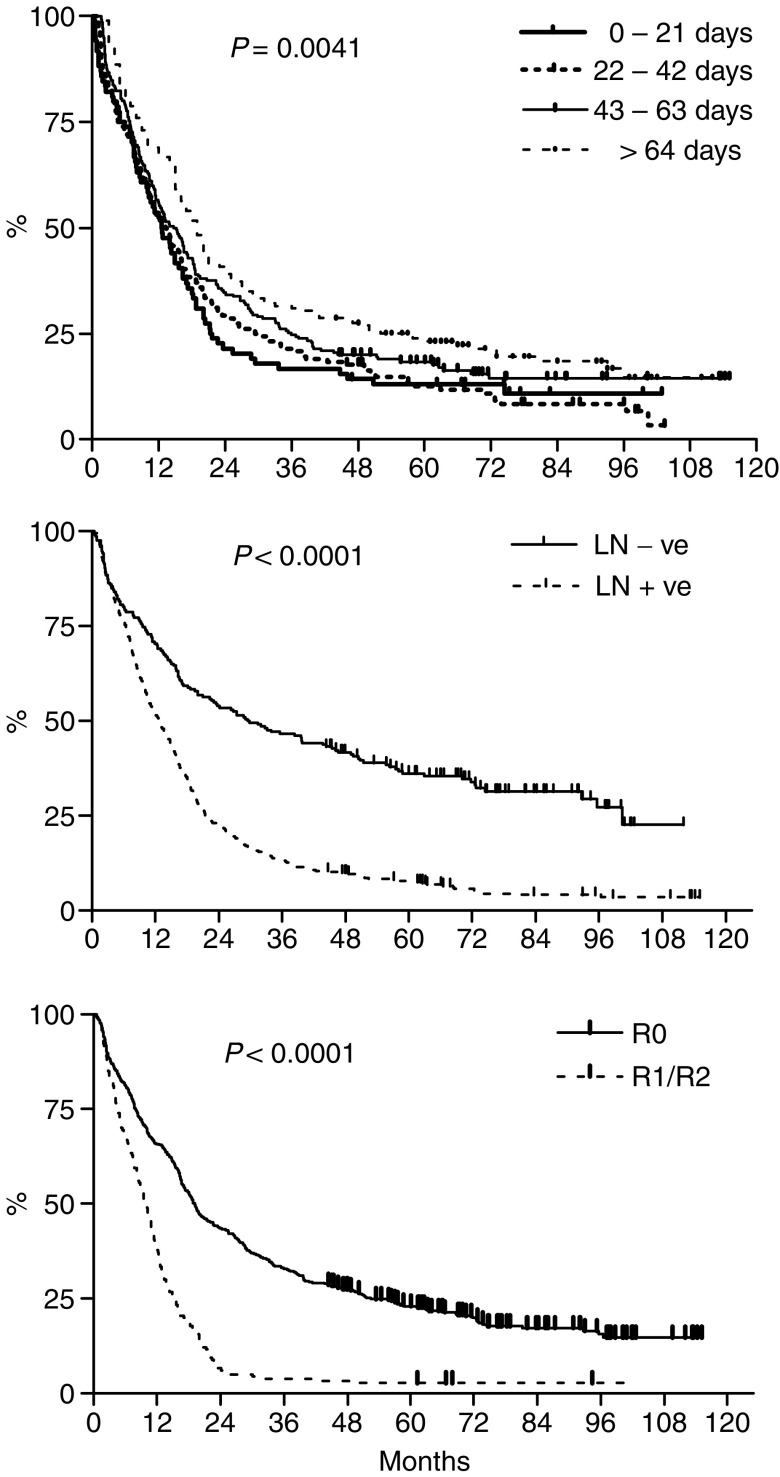
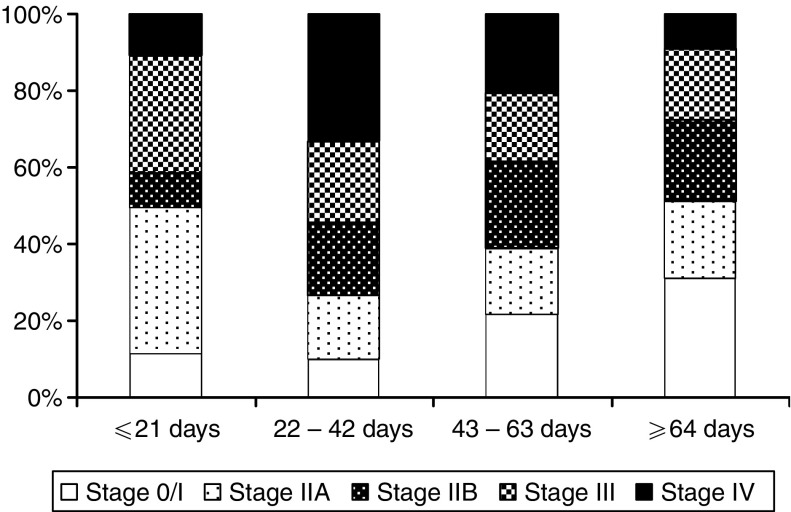
This retrospective study investigates if delays between the diagnosis of cancer of the oesophagus and surgical resection influence long-term survival. Data held by the West Midlands Cancer Intelligence Unit on 800 patients who underwent oesophagectomy for a diagnosis of cancer of the oesophagus or oesophagogastric junction between 1995 and 2000 were reviewed. Six hundred and thirty-two patients treated with curative intention and who had not received neo-adjuvant treatment in the form of radio- or chemotherapy were included in the analysis. The time interval between histological diagnosis and surgical resection was stratified into four groups: less than 3, 3-6, 6-9 and more than 9 weeks. The Cox proportional hazard model was used to test for the independent effect of delays. The results showed no difference in long-term survival according to the delay between histological diagnosis and surgical resection. On multivariate analysis adverse prognostic factors were advanced age, incomplete resection and lymph node involvement. Patients with a longer delay had a higher rate of complete tumour resection suggesting that they were more appropriately selected for the surgical treatment approach. In conclusion we have found no evidence that shorter delays from the date of histological diagnosis to surgical resection are beneficial to long-term survival.
这项回顾性研究调查了食管癌诊断与手术切除之间的延迟是否会影响长期生存率。对西米德兰兹癌症情报部门保存的1995年至2000年间因食管癌或食管胃交界部癌接受食管切除术的800例患者的数据进行了回顾。分析纳入了632例接受根治性治疗且未接受放疗或化疗形式的新辅助治疗的患者。组织学诊断与手术切除之间的时间间隔分为四组:少于3周、3 - 6周、6 - 9周和超过9周。采用Cox比例风险模型来检验延迟的独立影响。结果显示,根据组织学诊断与手术切除之间的延迟情况,长期生存率没有差异。多因素分析显示,不良预后因素为高龄、切除不完全和淋巴结受累。延迟时间较长的患者肿瘤完全切除率较高,这表明他们更适合选择手术治疗方法。总之,我们没有发现证据表明从组织学诊断日期到手术切除的较短延迟对长期生存有益。