Koppie Theresa M, Bianco Fernando J, Kuroiwa Kentaro, Reuter Victor E, Guillonneau Bertrand, Eastham James A, Scardino Peter T
Department of Urology, Memorial Sloan Kettering Cancer Center, New York, NY 10021, USA.
BJU Int. 2006 Dec;98(6):1167-71. doi: 10.1111/j.1464-410X.2006.06578.x. Epub 2006 Oct 9.
To identify the clinical characteristics of anterior prostate cancers (APCs) and to compare these with posterior prostate cancers (PPCs).
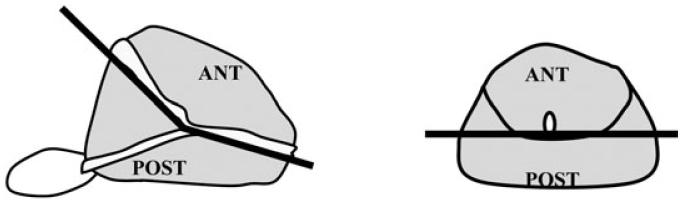
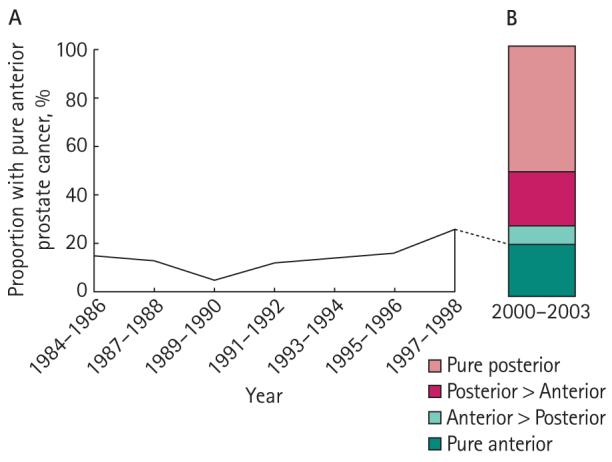
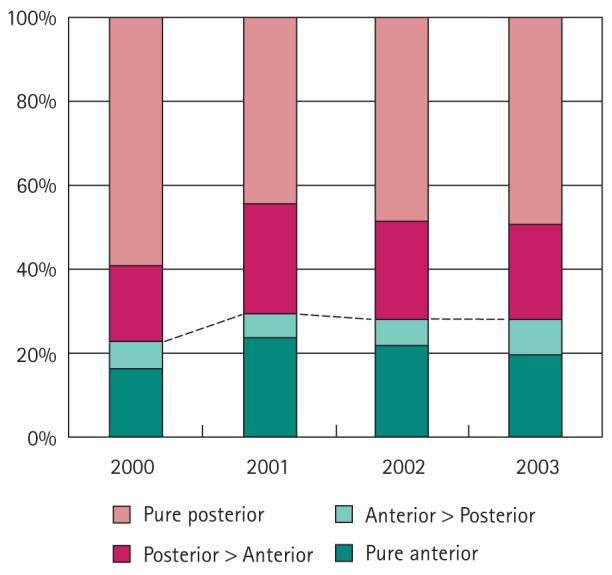
We reviewed 1290 consecutive open and laparoscopic radical prostatectomies (RPs) at the authors' institution from January 2000 to March 2004. Prostates were processed using a whole-mount technique. Each surgical specimen was reviewed by one pathologist, and tumour areas were marked, measured and mapped. Positive surgical margins (PSMs) were defined as the presence of cancer cells at the inked surface of the specimen. Specimens were then categorized by the location of their dominant tumour, i.e. pure anterior, anterior > posterior, posterior > anterior, or pure posterior. We compared the clinical and pathological characteristics of 259 patients in the pure-anterior group with the 594 in the pure-posterior group.
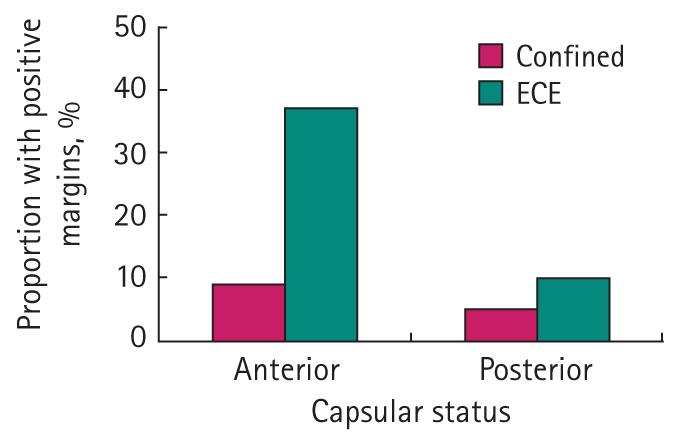
Before RP, APCs had a significantly lower biopsy Gleason score (78% vs 68% with Gleason 4-6), fewer mean biopsy cores positive (2.0 vs 2.6), a smaller median percentage of positive cores (17% vs 26%), lower clinical stage (T1 in 79% vs 62%), and higher progression-free probability estimated by preoperative nomogram (86% vs 84%) than PPCs. Patients with APCs also had more previous negative biopsy sessions. The pathological analysis of RP specimens showed that those with APCs had higher tumour volume (1.6 vs 0.83 mL) and had a higher PSM rate (12% vs 7%) than those with PPCs, despite specimens with PPCs having higher rates of extraprostatic extension (10% vs 19%).
APCs have lower Gleason grade and lower rates of extraprostatic extension, yet patients with anterior tumours have higher overall tumour volumes and higher PSM rates. Because current tools for detecting and staging prostate cancer can underestimate the extent of anterior prostate disease, improved methods are needed for localizing and characterizing anterior cancers.
确定前列腺前部癌(APC)的临床特征,并将其与前列腺后部癌(PPC)进行比较。
我们回顾了2000年1月至2004年3月在作者所在机构进行的1290例连续开放性和腹腔镜根治性前列腺切除术(RP)。前列腺采用全切片技术处理。每个手术标本由一名病理学家进行检查,标记、测量并绘制肿瘤区域。阳性手术切缘(PSM)定义为标本墨染表面存在癌细胞。然后根据主要肿瘤的位置对标本进行分类,即纯前部、前部>后部、后部>前部或纯后部。我们比较了纯前部组259例患者与纯后部组594例患者的临床和病理特征。
在RP术前,APC的活检Gleason评分显著较低(Gleason 4 - 6分者分别为78%和68%),平均活检阳性芯数较少(分别为2.0和2.6),阳性芯数的中位数百分比较小(分别为17%和26%),临床分期较低(T1期分别为79%和62%),术前列线图估计的无进展概率较高(分别为86%和84%),高于PPC。APC患者之前的活检阴性次数也更多。RP标本的病理分析显示,尽管PPC标本的前列腺外侵犯率较高(分别为10%和19%),但APC患者的肿瘤体积更大(分别为1.6和0.83 mL),PSM率更高(分别为12%和7%)。
APC的Gleason分级较低,前列腺外侵犯率较低,但前部肿瘤患者的总体肿瘤体积较大,PSM率较高。由于目前检测和分期前列腺癌的工具可能会低估前列腺前部疾病的范围,因此需要改进方法来定位和表征前部癌症。