Gimbel-Sherr Sarah O, Micek Mark A, Gimbel-Sherr Kenneth H, Koepsell Thomas, Hughes James P, Thomas Katherine K, Pfeiffer James, Gloyd Stephen S
Department of Epidemiology, Box 357236, School of Public Health and Community Medicine, University of Washington, Seattle, WA 98195, USA.
Hum Resour Health. 2007 Feb 28;5:7. doi: 10.1186/1478-4491-5-7.
The most pressing challenge to achieving universal access to highly active anti-retroviral therapy (HAART) in sub-Saharan Africa is the shortage of trained personnel to handle the increased service requirements of rapid roll-out. Overcoming the human resource challenge requires developing innovative models of care provision that improve efficiency of service delivery and rationalize use of limited resources.
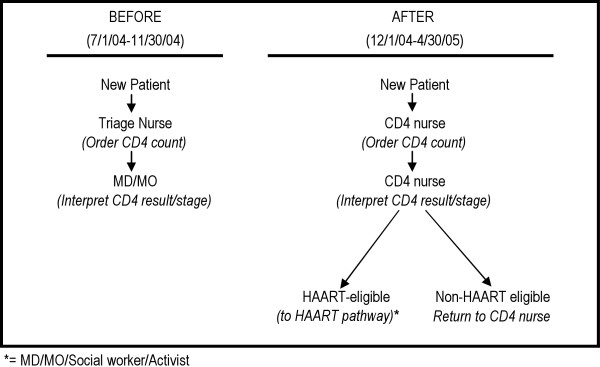
We conducted a time-series intervention trial in two HIV clinics in central Mozambique to discern whether expanding the role of basic-level nurses to stage HIV-positive patients using CD4 counts and WHO-defined criteria would lead to more rapid information on patient status (including identification of HAART eligible patients), increased efficiency in the use of higher-level clinical staff, and increased capacity to start HAART-eligible patients on treatment.
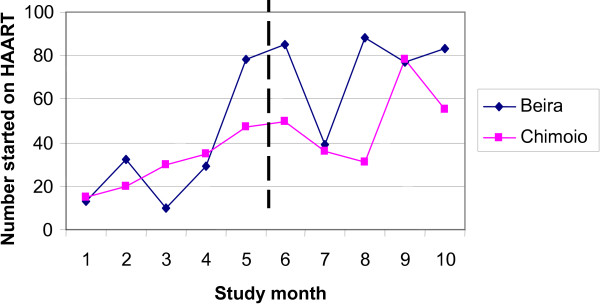
Overall, 1,880 of the HAART-eligible patients were considered in the study of whom 48.5% started HAART, with a median time of 71 days from their initial blood draw. After adjusting for time, expanding the role of nurses to stage patients was associated with more rational use of higher-level clinical staff at one site (Beira OR 1.9, 95% CI 1.1-3.3; Chimoio OR 0.2, 95% CI 0.1-0.5). In multivariate analyses, the rate of starting HAART in patients with CD4 counts of less than 200/mm3 increased over time (HR = 1.07, 95% CI 1.02-1.13), as did the total number of new patients initiating HAART (beta = 7.3, 95% CI 1.3-13.3). However, the intervention was not independently associated with either of these outcomes in multivariate analyses (HR = 0.9, 95% CI 0.7-1.2) for starting HAART in patients with CD4 counts of less than 200/mm3; (beta = -5.2, p = 0.75) for the total number of new patients initiating HAART per month. No effect of the intervention was found in these outcomes when stratifying by site.
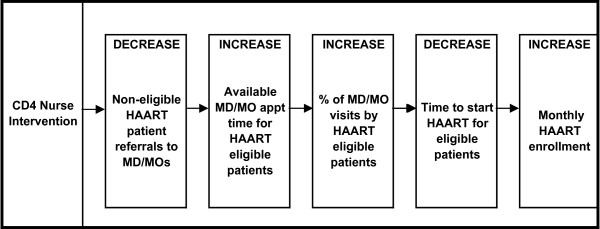
The CD4 nurse intervention, when implemented correctly, was associated with a more rational use of higher-level clinical providers, which may improve overall clinic flow and efficient use of the limited supply of human resources. However, this intervention did not lead to an increase in the number of patients starting HAART or a reduction in the time to HAART initiation. Study month appears to play an important role in all outcomes, suggesting that general improvements in clinic efficiency may have overshadowed the effect of the intervention. The lack of observed effect in these outcomes may be due to additional health systems bottlenecks that delay the initiation of treatment in HAART-eligible patients.
在撒哈拉以南非洲地区,实现普遍获得高效抗逆转录病毒疗法(HAART)面临的最紧迫挑战是缺乏训练有素的人员来应对快速推广带来的服务需求增加。克服人力资源挑战需要开发创新的护理模式,以提高服务提供效率并合理利用有限资源。
我们在莫桑比克中部的两家艾滋病毒诊所进行了一项时间序列干预试验,以确定扩大基层护士使用CD4计数和世界卫生组织定义的标准对艾滋病毒阳性患者进行分期的作用是否会带来关于患者状况的更快信息(包括确定符合HAART治疗条件的患者)、提高高级临床工作人员的使用效率以及增加为符合HAART治疗条件的患者开始治疗的能力。
总体而言,在该研究中考虑了1880名符合HAART治疗条件的患者,其中48.5%开始接受HAART治疗,从首次采血到开始治疗的中位时间为71天。在对时间进行调整后,在一个地点(贝拉,比值比1.9,95%置信区间1.1 - 3.3;希莫尤,比值比0.2,95%置信区间0.1 - 0.5),扩大护士对患者进行分期的作用与更合理地使用高级临床工作人员相关。在多变量分析中,CD4计数低于200/mm³的患者开始接受HAART治疗的比例随时间增加(风险比 = 1.07,95%置信区间1.02 - 1.13),开始接受HAART治疗的新患者总数也增加(β = 7.3,95%置信区间1.3 - 13.3)。然而,在多变量分析中,对于CD4计数低于200/mm³的患者开始接受HAART治疗(风险比 = 0.9,95%置信区间0.7 - 1.2)以及每月开始接受HAART治疗的新患者总数(β = -5.2,p = 0.75),该干预与这些结果均无独立关联。按地点分层时,在这些结果中未发现该干预有任何效果。
CD4护士干预若正确实施,与更合理地使用高级临床提供者相关,这可能改善整体诊所流程并有效利用有限的人力资源。然而,该干预并未导致开始接受HAART治疗的患者数量增加或HAART治疗启动时间缩短。研究月份似乎在所有结果中都起着重要作用,这表明诊所效率的总体提高可能掩盖了干预的效果。在这些结果中未观察到效果可能是由于其他卫生系统瓶颈导致符合HAART治疗条件的患者延迟开始治疗。