Division of General Internal Medicine, San Francisco General Hospital, Department of Medicine, University of California, San Francisco (UCSF), San Francisco, CA, USA.
Kenya Medical Research Institute, Nairobi, Kenya.
Implement Sci. 2017 Aug 8;12(1):102. doi: 10.1186/s13012-017-0630-8.
The global response to HIV has started over 18 million persons on life-saving antiretroviral therapy (ART)-the vast majority in low- and middle-income countries (LMIC)-yet substantial gaps remain: up to 40% of persons living with HIV (PLHIV) know their status, while another 30% of those who enter care are inadequately retained after starting treatment. Identifying strategies to enhance use of treatment is urgently needed, but the conceptualization and specification of implementation interventions is not always complete. We sought to assess the completeness of intervention reporting in research to advance uptake of treatment for HIV globally.
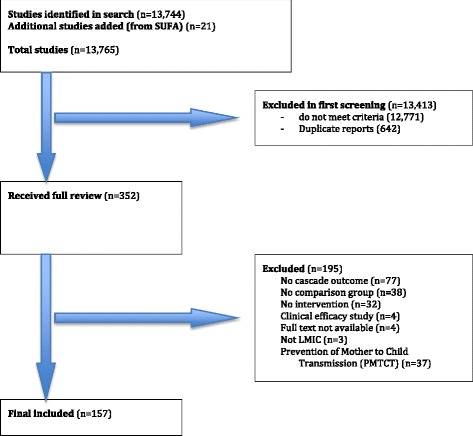
We carried out a systematic review to identify interventions targeting the adult HIV care cascade in LMIC dating from 1990 to 2017. We identified components of each intervention as "intervention types" to decompose interventions into common components. We grouped "intervention types" into a smaller number of more general "implementation approaches" to aid summarization. We assessed the reporting of six intervention characteristics adapted from the implementation science literature: the actor, action, action dose, action temporality, action target, and behavioral target in each study.
In 157 unique studies, we identified 34 intervention "types," which were empirically grouped into six generally understandable "approaches." Overall, 42% of interventions defined the actor, 64% reported the action, 41% specified the intervention "dose," 43% reported action temporality, 61% defined the action target, and 69% reported a target behavior. Average completeness of reporting varied across approaches from a low of 50% to a high of 72%. Dimensions that involved conceptualization of the practices themselves (e.g., actor, dose, temporality) were in general less well specified than consequences (e.g., action target and behavioral target).
The conceptualization and Reporting of implementation interventions to advance treatment for HIV in LMIC is not always complete. Dissemination of standards for reporting intervention characteristics can potentially promote transparency, reproducibility, and scientific accumulation in the area of implementation science to address HIV in low- and middle-income countries.
全球应对艾滋病的行动已使超过 1800 万人接受了挽救生命的抗逆转录病毒疗法(ART)——绝大多数在中低收入国家(LMIC)——但仍存在巨大差距:多达 40%的艾滋病毒感染者(PLHIV)知晓自己的状况,而在开始治疗后,另有 30%的进入护理的人无法得到充分的保留。迫切需要确定加强治疗使用的策略,但实施干预措施的概念化和具体说明并不总是完整的。我们试图评估研究中针对中低收入国家艾滋病护理级联的干预措施报告的完整性,以推动全球接受艾滋病治疗。
我们进行了一项系统综述,以确定自 1990 年至 2017 年针对中低收入国家成年艾滋病毒护理级联的干预措施。我们将每项干预措施的组成部分确定为“干预类型”,将干预措施分解为常见组成部分。我们将“干预类型”分组为少数更通用的“实施方法”,以帮助总结。我们评估了从实施科学文献中改编的六个干预特征的报告:在每项研究中,参与者、行动、行动剂量、行动时间性、行动目标和行为目标。
在 157 项独特的研究中,我们确定了 34 种干预“类型”,这些类型在经验上被分为六个易于理解的“方法”。总体而言,42%的干预措施确定了参与者,64%报告了行动,41%具体说明了干预“剂量”,43%报告了行动时间性,61%定义了行动目标,69%报告了目标行为。报告方法的平均完整性从低至 50%到高至 72%不等。涉及实践本身概念化的维度(例如,参与者、剂量、时间性)通常不如后果(例如,行动目标和行为目标)规定得那么详细。
在中低收入国家推进艾滋病治疗的实施干预措施的概念化和报告并不总是完整的。传播干预特征报告的标准可能会促进实施科学领域的透明度、可重复性和科学积累,以解决中低收入国家的艾滋病问题。