Department of Radiation Oncology, University Hospital Zurich, Rämistrasse 100, 8091 Zurich, Switzerland.
Radiat Oncol. 2007 Apr 12;2:16. doi: 10.1186/1748-717X-2-16.
Except for early T1,2 N0 stages, the prognosis for patients with oral cavity cancer (OCC) is reported to be worse than for carcinoma in other sites of the head and neck (HNC). The aim of this work was to assess disease outcome in OCC following IMRT.Between January 2002 and January 2007, 346 HNC patients have been treated with curative intensity modulated radiation therapy (IMRT) at the Department of Radiation Oncology, University Hospital Zurich. Fifty eight of these (16%) were referred for postoperative (28) or definitive (30) radiation therapy of OCC.40 of the 58 OCC patients (69%) presented with locally advanced T3/4 or recurred lesions. Doses between 60 and 70 Gy were applied, combined with simultaneous cisplatin based chemotherapy in 78%. Outcome analyses were performed using Kaplan Meier curves.In addition, comparisons were performed between this IMRT OCC cohort and historic in-house cohorts of 33 conventionally irradiated (3DCRT) and 30 surgery only patients treated over the last 10 years.
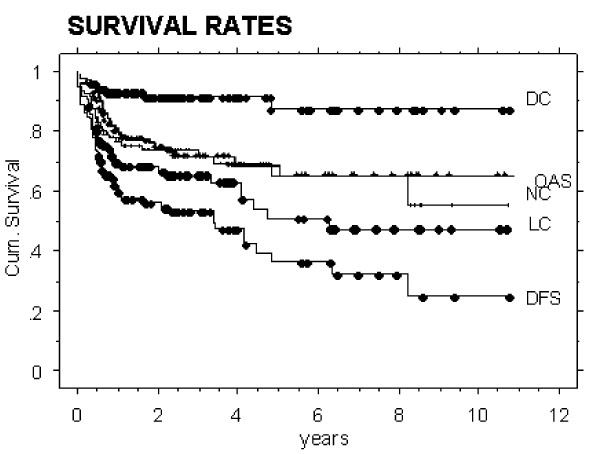
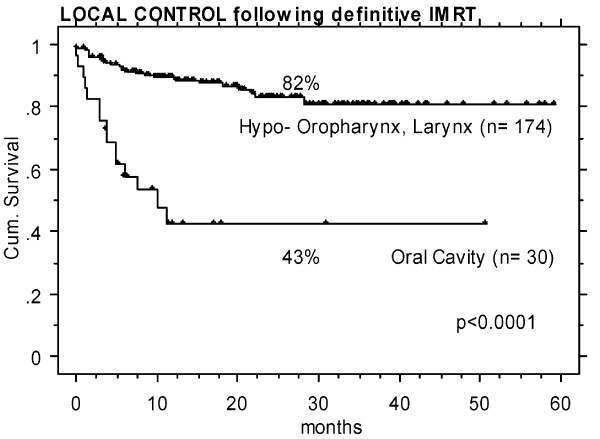
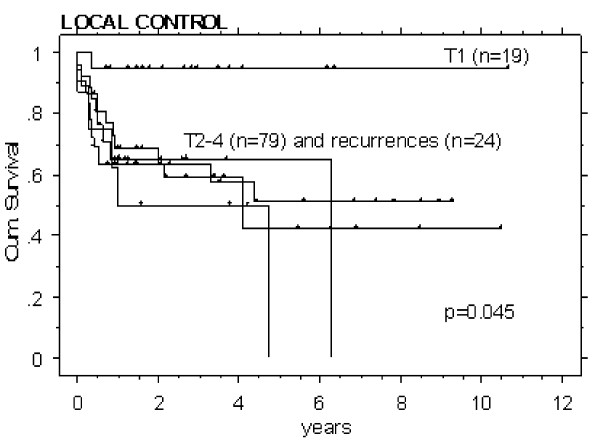
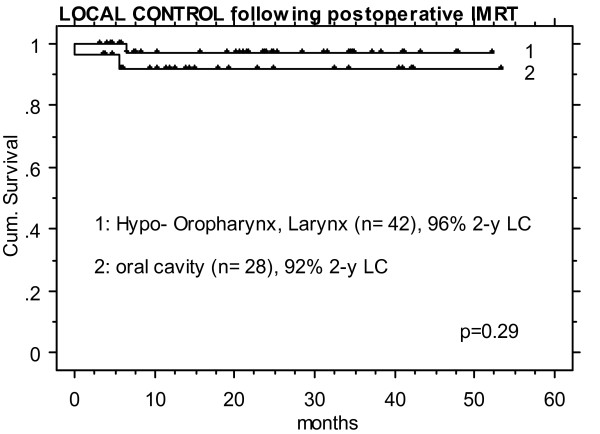
OCC patients treated with postoperative IMRT showed the highest local control (LC) rate of all assessed treatment sequence subgroups (92% LC at 2 years). Historic postoperative 3DCRT patients and patients treated with surgery alone reached LC rates of approximately 70-80%. Definitively irradiated patients revealed poorest LC rates with approximately 30 and 40% following 3DCRT and IMRT, respectively.T1 stage resulted in an expectedly significantly higher LC rate (95%, n = 19, p < 0.05) than T2-4 and recurred stages (LC approximately 50-60%, n = 102).Analyses according to the diagnosis revealed significantly lower LC in OCC following definitive IMRT than that in pharyngeal tumors treated with definitive IMRT in the same time period (43% vs 82% at 2 years, p < 0.0001), while the LC rate of OCC following postoperative IMRT was as high as in pharyngeal tumors treated with postoperative IMRT (>90% at 2 years).
Postoperative IMRT of OCC resulted in the highest local control rate of the assessed treatment subgroups. In conclusion, generous indication for IMRT following surgical treatment is recommended in OCC cases with unfavourable features like tight surgical margin, nodal involvement, primary tumor stage >T1N0, or already recurred disease, respectively.Loco-regional outcome of OCC following definitive IMRT remained unsatisfactory, comparable to that following definitive 3DCRT.
除了早期 T1、2 N0 期外,口腔癌 (OCC) 患者的预后被报道比头颈部 (HNC) 其他部位的癌症更差。本研究旨在评估调强放疗 (IMRT) 后 OCC 的疾病转归。
2002 年 1 月至 2007 年 1 月,苏黎世大学医院放射肿瘤学系对 346 例 HNC 患者进行了根治性调强放疗 (IMRT)。其中 58 例 (16%)为 OCC 术后 (28 例) 或根治性 (30 例) 放疗。58 例 OCC 患者中有 40 例 (69%)为局部晚期 T3/4 或复发。应用 60-70Gy 剂量,78%患者同时给予顺铂为基础的化疗。采用 Kaplan-Meier 曲线进行生存分析。此外,将该组 OCC 患者与过去 10 年中 33 例接受常规放疗 (3DCRT) 和 30 例单纯手术治疗的回顾性组内队列进行比较。
术后接受 IMRT 的 OCC 患者在所有评估的治疗顺序亚组中局部控制率最高 (2 年时局部控制率为 92%)。回顾性分析术后 3DCRT 患者和单纯手术患者的局部控制率约为 70-80%。接受根治性放疗的患者局部控制率最差,3DCRT 和 IMRT 后分别约为 30%和 40%。T1 期患者的局部控制率明显高于 T2-4 期和复发期 (95%,n=19,p<0.05)。按诊断分析显示,同期接受根治性 IMRT 的下咽肿瘤局部控制率明显低于 OCC (2 年时为 43% vs 82%,p<0.0001),而术后接受 IMRT 的 OCC 局部控制率与同期接受术后 IMRT 的下咽肿瘤相似 (>90%,2 年时)。
OCC 的术后 IMRT 治疗获得了评估治疗亚组中最高的局部控制率。因此,对于具有不良特征的 OCC 病例,如手术切缘紧张、淋巴结受累、原发肿瘤分期>T1N0 或已经复发的患者,建议给予 IMRT 治疗。OCC 患者接受根治性 IMRT 后的局部区域疗效仍不理想,与接受根治性 3DCRT 后的疗效相当。