Marcin James P, Dharmar Madan, Cho Meyng, Seifert Lynn L, Cook Jenifer L, Cole Stacey L, Nasrollahzadeh Farid, Romano Patrick S
Department of Pediatrics, University of California-Davis, Sacramento, CA 95817, USA.
Ann Emerg Med. 2007 Oct;50(4):361-7, 367.e1-2. doi: 10.1016/j.annemergmed.2007.01.020. Epub 2007 Apr 11.
We identify the incidence, nature, and consequences of medication errors among acutely ill and injured children receiving care in a sample of rural emergency departments (EDs).
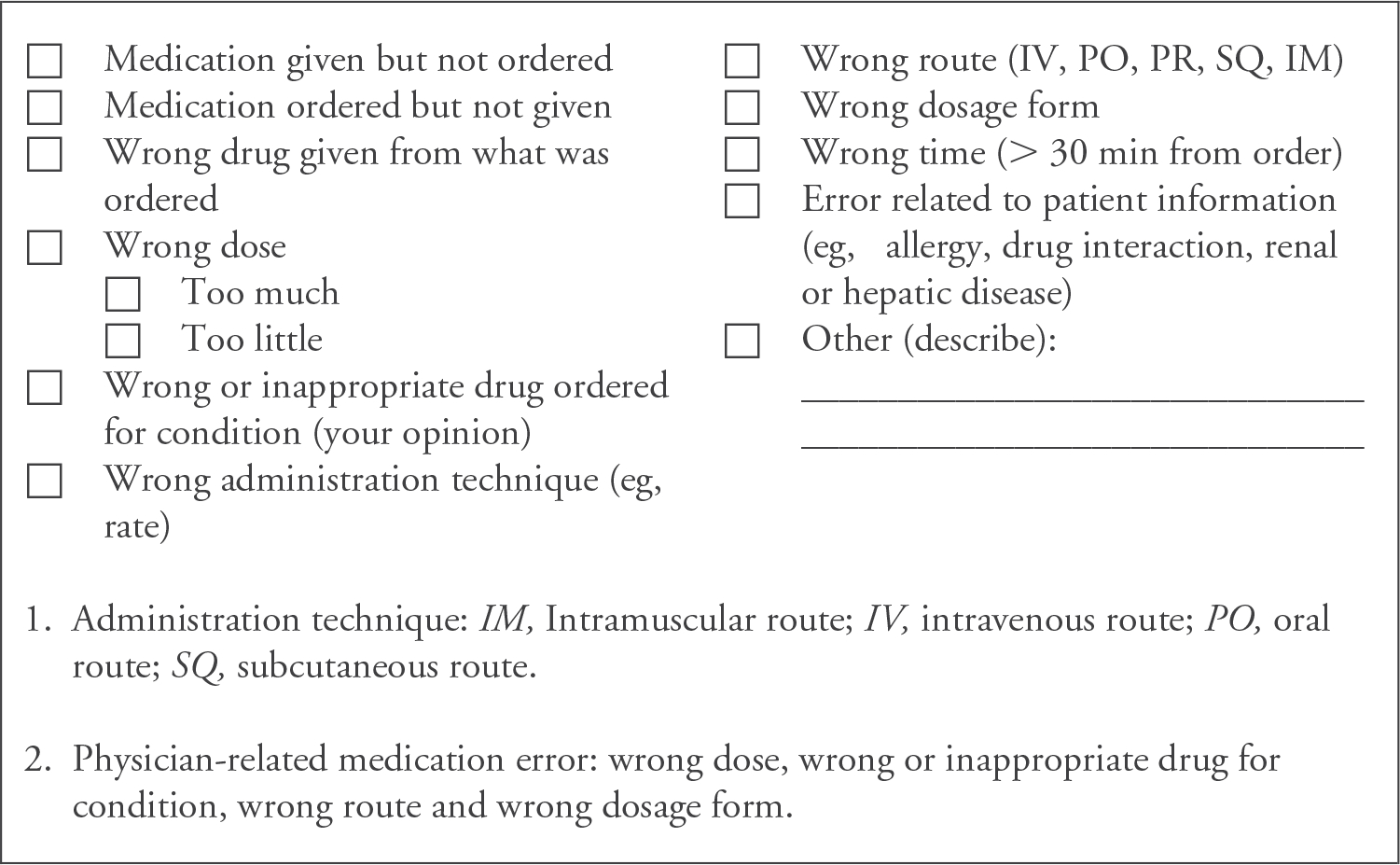
Two pediatric pharmacists applied a medication error data collection instrument to the medical records of all critically ill children (highest triage category) treated in 4 northern California rural EDs between January 2000 and June 2003. Physician-related medication errors were defined as those involving wrong dose, wrong or inappropriate medication for condition, wrong route, or wrong dosage form. Wrong dose was determined by preset criteria, with doses above or below 10% to 25% of correct dose considered errors, depending on class of medication. Medication errors were classified into categories A through I under 3 broader categories, including errors having the potential to cause harm (A), errors that cause no harm (B to D), and errors that cause harm to the patient (E to I).
Complete data were available from 177 (97.3%) of the 182 patients identified as having been triaged in the highest category during the study period. A total of 84 medication errors were identified among 69 patients, resulting in a medication error incidence of 39.0%. Twenty-four physician-related medication errors were identified among 21 patients, resulting in a physician-related medication error incidence of 11.9%. Among the 69 patients with medication errors, 11 had errors categorized as having the potential to cause harm (15.9%), and 58 had errors categorized as causing no harm (85.5%).
We found a high incidence of medication errors and physician-related medication errors among the acutely ill and injured children presenting to rural EDs in northern California. None of the medication errors identified caused harm to the patients included in this study.
我们确定在农村急诊科样本中接受治疗的急病和受伤儿童用药错误的发生率、性质及后果。
两名儿科药剂师将用药错误数据收集工具应用于2000年1月至2003年6月期间在加利福尼亚州北部4家农村急诊科接受治疗的所有重症儿童(最高分诊类别)的病历。与医生相关的用药错误定义为涉及剂量错误、针对病情的药物错误或不当、给药途径错误或剂型错误。剂量错误由预设标准确定,根据药物类别,高于或低于正确剂量10%至25%的剂量被视为错误。用药错误分为A至I类,在3个更广泛的类别中,包括有可能造成伤害的错误(A)、未造成伤害的错误(B至D)以及对患者造成伤害的错误(E至I)。
在研究期间被确定为最高分诊类别的182名患者中,有177名(97.3%)获得了完整数据。在69名患者中总共发现了84起用药错误,用药错误发生率为39.0%。在21名患者中发现了24起与医生相关的用药错误,与医生相关的用药错误发生率为11.9%。在69名有用药错误的患者中,11名患者的错误被归类为有可能造成伤害(15.9%),58名患者的错误被归类为未造成伤害(85.5%)。
我们发现在加利福尼亚州北部农村急诊科就诊的急病和受伤儿童中,用药错误及与医生相关的用药错误发生率很高。本研究中发现的用药错误均未对纳入研究的患者造成伤害。