Bozza Fernando A, Salluh Jorge I, Japiassu André M, Soares Marcio, Assis Edson F, Gomes Rachel N, Bozza Marcelo T, Castro-Faria-Neto Hugo C, Bozza Patrícia T
ICU, Instituto de Pesquisa Clínica Evandro Chagas, Fundação Oswaldo Cruz, Av Brasil 4365, Rio de Janeiro, Brazil.
Crit Care. 2007;11(2):R49. doi: 10.1186/cc5783.
The current shortage of accurate and readily available, validated biomarkers of disease severity in sepsis is an important limitation when attempting to stratify patients into homogeneous groups, in order to study pathogenesis or develop therapeutic interventions. The aim of the present study was to determine the cytokine profile in plasma of patients with severe sepsis by using a multiplex system for simultaneous detection of 17 cytokines.
This was a prospective cohort study conducted in four tertiary hospitals. A total of 60 patients with a recent diagnosis of severe sepsis were included. Plasma samples were collected for measurement of cytokine concentrations. A multiplex analysis was performed to evaluate levels of 17 cytokines (IL-1 beta, IL-2, IL-4, IL-5, IL-6, IL-7, IL-8, IL-10, IL-12, IL-13, IL-17, interferon-gamma, granulocyte colony-stimulating factor [G-CSF], granulocyte-macrophage colony-stimulating factor, monocyte chemoattractant protein [MCP]-1, macrophage inflammatory protein-1 and tumour necrosis factor-alpha). Cytokine concentrations were related to the presence of severe sepsis or septic shock, the severity and evolution of organ failure, and early and late mortality.
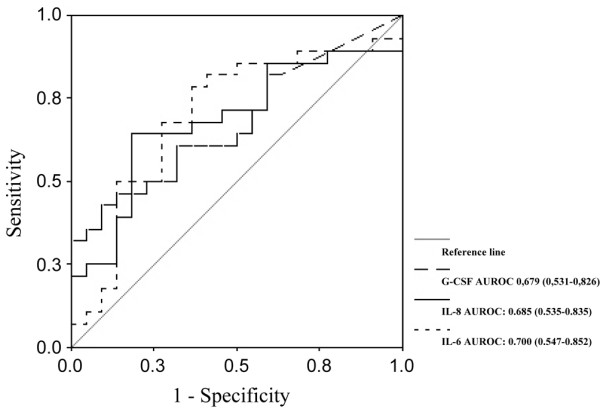
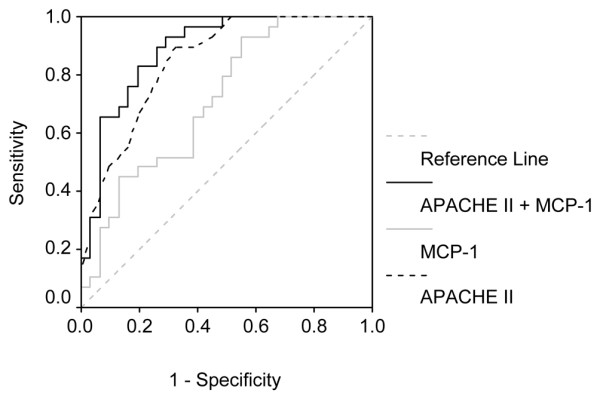
Concentrations of IL-1 beta, IL-6, IL-7, IL-8, IL-10, IL-13, interferon-gamma, MCP-1 and tumour necrosis factor-alpha were significantly higher in septic shock patients than in those with severe sepsis. Cytokine concentrations were associated with severity and evolution of organ dysfunction. With regard to the severity of organ dysfunction on day 1, IL-8 and MCP-1 exhibited the best correlation with Sequential Organ Failure Assessment score. In addition, IL-6, IL-8 and G-CSF concentrations during the first 24 hours were predictive of worsening organ dysfunction or failure of organ dysfunction to improve on day three. In terms of predicting mortality, the cytokines IL-1 beta, IL-4, IL-6, IL-8, MCP-1 and G-CSF had good accuracy for predicting early mortality (< 48 hours), and IL-8 and MCP-1 had the best accuracy for predicting mortality at 28 days. In multivariate analysis, only MCP-1 was independently associated with prognosis.
In this exploratory analysis we demonstrated that use of a multiple cytokine assay platform allowed identification of distinct cytokine profiles associated with sepsis severity, evolution of organ failure and death.
目前在脓毒症中缺乏准确、现成且经过验证的疾病严重程度生物标志物,这在试图将患者分层为同质组以研究发病机制或开发治疗干预措施时是一个重要限制。本研究的目的是通过使用多重系统同时检测17种细胞因子来确定严重脓毒症患者血浆中的细胞因子谱。
这是一项在四家三级医院进行的前瞻性队列研究。共纳入60例近期诊断为严重脓毒症的患者。采集血浆样本以测量细胞因子浓度。进行多重分析以评估17种细胞因子(白细胞介素-1β、白细胞介素-2、白细胞介素-4、白细胞介素-5、白细胞介素-6、白细胞介素-7、白细胞介素-8、白细胞介素-10、白细胞介素-12、白细胞介素-13、白细胞介素-17、干扰素-γ、粒细胞集落刺激因子[G-CSF]、粒细胞-巨噬细胞集落刺激因子、单核细胞趋化蛋白[MCP]-1、巨噬细胞炎性蛋白-1和肿瘤坏死因子-α)的水平。细胞因子浓度与严重脓毒症或脓毒性休克的存在、器官功能衰竭的严重程度和演变以及早期和晚期死亡率相关。
脓毒性休克患者血浆中白细胞介素-1β、白细胞介素-6、白细胞介素-7、白细胞介素-8、白细胞介素-10、白细胞介素-13、干扰素-γ、MCP-1和肿瘤坏死因子-α的浓度显著高于严重脓毒症患者。细胞因子浓度与器官功能障碍的严重程度和演变相关。关于第1天器官功能障碍的严重程度,白细胞介素-8和MCP-1与序贯器官衰竭评估评分的相关性最佳。此外,最初24小时内白细胞介素-6、白细胞介素-8和G-CSF的浓度可预测第3天器官功能障碍的恶化或器官功能障碍无法改善。在预测死亡率方面,白细胞介素-1β、白细胞介素-4、白细胞介素-6、白细胞介素-8、MCP-1和G-CSF这些细胞因子对预测早期死亡率(<48小时)具有良好的准确性,而白细胞介素-8和MCP-1对预测28天死亡率的准确性最佳。在多变量分析中,只有MCP-1与预后独立相关。
在这项探索性分析中,我们证明使用多重细胞因子检测平台能够识别与脓毒症严重程度、器官衰竭演变和死亡相关的不同细胞因子谱。