Hutchison Colin A, Crowe Alex V, Stevens Paul E, Harrison David A, Lipkin Graham W
University Hospital Birmingham NHS Foundation Trust, Queen Elizabeth Medical Centre, Edgbaston, Birmingham, B15 2TH, UK.
Crit Care. 2007;11(2):R50. doi: 10.1186/cc5785.
This report describes the case mix, outcome and activity for admissions to intensive care units (ICUs) of patients who require prior chronic renal dialysis for end-stage renal failure (ESRF), and investigates the effect of case mix factors on outcome.
This was a secondary analysis of a high-quality clinical database, namely the Intensive Care National Audit & Research Centre (ICNARC) Case Mix Programme Database, which includes 276,731 admissions to 170 adult ICUs across England, Wales and Northern Ireland from 1995 to 2004.
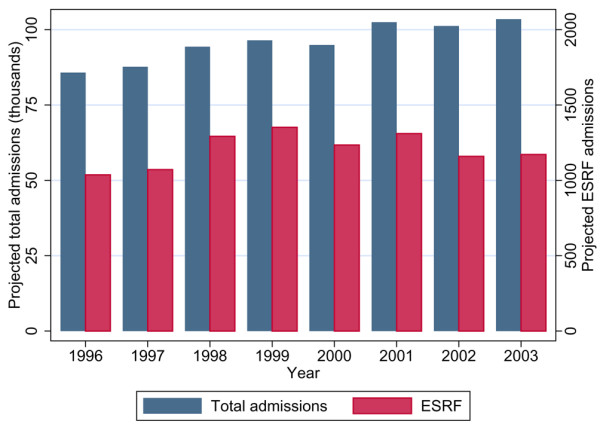
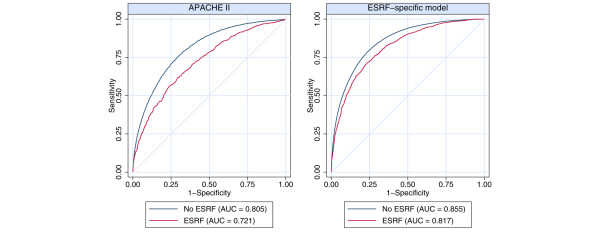
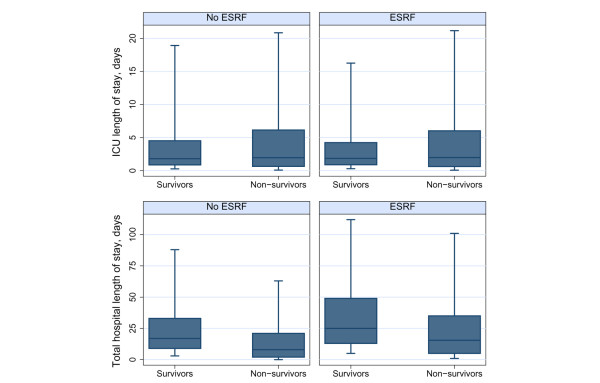
During the eight year study period, 1.3% (n = 3,420) of all patients admitted to ICU were receiving chronic renal dialysis before ICU admission. This represents an estimated ICU utilization of six admissions (32 bed-days) per 100 dialysis patient-years. The ESRF group was younger (mean age 57.3 years versus 59.5 years) and more likely to be male (60.2% versus 57.9%) than those without ESRF. Acute Physiology and Chronic Health Evaluation II score and Acute Physiology Score revealed greater severity of illness on admission in patients with ESRF (mean 24.7 versus 16.6 and 17.2 versus 12.6, respectively). Length of stay in ICU was comparable between groups (median 1.9 days versus 1.8 days) and ICU mortality was only slightly elevated in the ESRF group (26.3% versus 20.8%). However, the ESRF group had protracted overall hospital stay (median 25 days versus 17 days), and increased hospital mortality (45.3% versus 31.2%) and ICU readmission (9.0% vs. 4.7%). Multiple logistic regression analysis adjusted for case mix identified the increased hospital mortality to be associated with increasing age, emergency surgery and nonsurgical cases, cardiopulmonary resuscitation before ICU admission and extremes of physiological norms. The adjusted odds ratio for ultimate hospital mortality associated with chronic renal dialysis was 1.24 (95% confidence interval 1.13 to 1.37).
Patients with ESRF admitted to UK ICUs are more likely to be male and younger, with a medical cause of admission, and to have greater severity of illness than the non-ESRF population. Outcomes on the ICU were comparable between the two groups, but those patients with ESRF had greater readmission rates, prolonged post-ICU hospital stay and increased post-ICU hospital mortality. This study is by far the largest comparative outcome analysis to date in patients with ESRF admitted to the ICU. It may help to inform clinical decision-making and resource requirements for this patient population.
本报告描述了因终末期肾衰竭(ESRF)而需要长期进行慢性肾透析的患者入住重症监护病房(ICU)的病例组合、治疗结果及医疗活动,并研究了病例组合因素对治疗结果的影响。
这是对一个高质量临床数据库进行的二次分析,该数据库即重症监护国家审计与研究中心(ICNARC)病例组合项目数据库,其中包含1995年至2004年期间英格兰、威尔士和北爱尔兰170个成人ICU的276,731例入院病例。
在为期八年的研究期间,所有入住ICU的患者中有1.3%(n = 3420)在入住ICU之前接受慢性肾透析治疗。这相当于每100个透析患者年中有6例(32个床日)入住ICU。与未患ESRF的患者相比,ESRF组患者更年轻(平均年龄57.3岁对59.5岁),且男性比例更高(60.2%对57.9%)。急性生理与慢性健康状况评价II评分(APACHE II)和急性生理评分(APS)显示,ESRF患者入院时病情严重程度更高(分别为平均24.7对16.6以及17.2对12.6)。两组患者在ICU的住院时间相当(中位数分别为1.9天和1.8天),ESRF组的ICU死亡率仅略有升高(26.3%对20.8%)。然而,ESRF组患者的总体住院时间延长(中位数为25天对17天),医院死亡率增加(45.3%对31.2%),ICU再入院率升高(9.0%对4.7%)。经病例组合调整的多因素logistic回归分析表明,医院死亡率增加与年龄增长、急诊手术和非手术病例、入住ICU前的心肺复苏以及生理指标的极端情况有关。与慢性肾透析相关的最终医院死亡率的调整比值比为1.24(95%置信区间为1.13至1.37)。
入住英国ICU的ESRF患者比未患ESRF的人群更可能为男性且更年轻,因内科疾病入院,病情严重程度更高。两组患者在ICU的治疗结果相当,但ESRF患者的再入院率更高,ICU后的住院时间延长,ICU后医院死亡率增加。本研究是迄今为止对入住ICU的ESRF患者进行的最大规模的比较性治疗结果分析。它可能有助于为该患者群体的临床决策和资源需求提供参考。