Division of Nephrology and Hypertension, Department of Medicine, University of North Carolina (UNC) Kidney Center, UNC School of Medicine, Chapel Hill, NC; Cecil G. Sheps Center for Health Services Research, University of North Carolina, Chapel Hill, NC.
Division of Nephrology and Hypertension, Department of Medicine, University of North Carolina (UNC) Kidney Center, UNC School of Medicine, Chapel Hill, NC.
Am J Kidney Dis. 2021 Feb;77(2):190-203.e1. doi: 10.1053/j.ajkd.2020.09.003. Epub 2020 Sep 19.
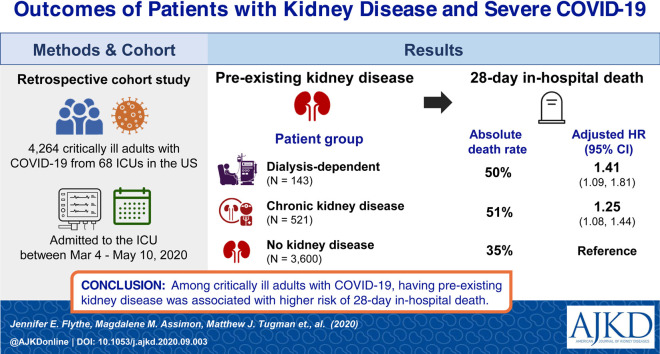
RATIONALE & OBJECTIVE: Underlying kidney disease is an emerging risk factor for more severe coronavirus disease 2019 (COVID-19) illness. We examined the clinical courses of critically ill COVID-19 patients with and without pre-existing chronic kidney disease (CKD) and investigated the association between the degree of underlying kidney disease and in-hospital outcomes.
Retrospective cohort study.
SETTINGS & PARTICIPANTS: 4,264 critically ill patients with COVID-19 (143 patients with pre-existing kidney failure receiving maintenance dialysis; 521 patients with pre-existing non-dialysis-dependent CKD; and 3,600 patients without pre-existing CKD) admitted to intensive care units (ICUs) at 68 hospitals across the United States.
PREDICTOR(S): Presence (vs absence) of pre-existing kidney disease.
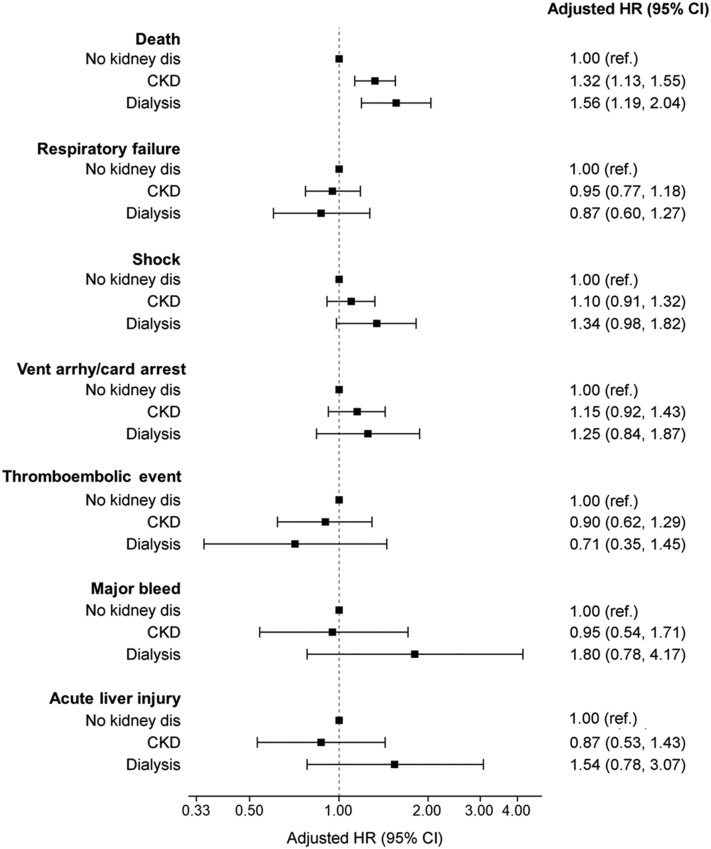
OUTCOME(S): In-hospital mortality (primary); respiratory failure, shock, ventricular arrhythmia/cardiac arrest, thromboembolic events, major bleeds, and acute liver injury (secondary).
We used standardized differences to compare patient characteristics (values>0.10 indicate a meaningful difference between groups) and multivariable-adjusted Fine and Gray survival models to examine outcome associations.
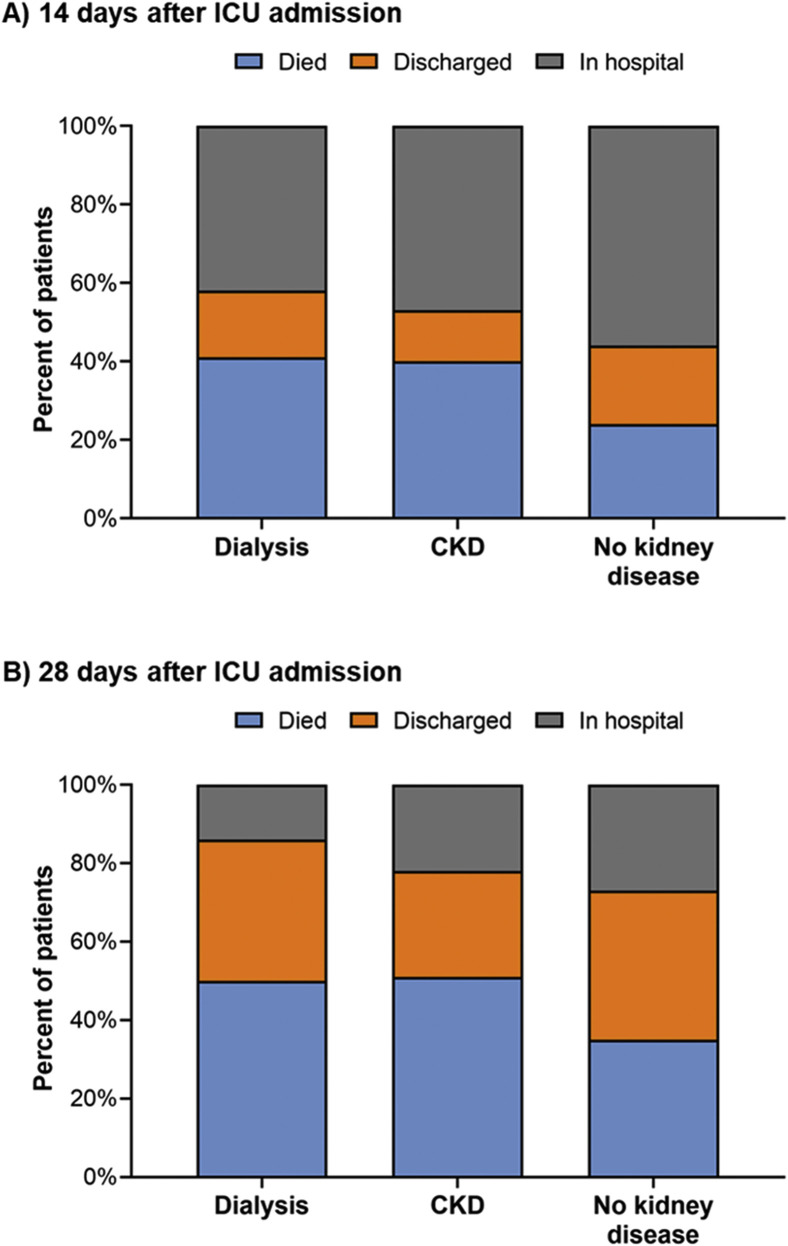
Dialysis patients had a shorter time from symptom onset to ICU admission compared to other groups (median of 4 [IQR, 2-9] days for maintenance dialysis patients; 7 [IQR, 3-10] days for non-dialysis-dependent CKD patients; and 7 [IQR, 4-10] days for patients without pre-existing CKD). More dialysis patients (25%) reported altered mental status than those with non-dialysis-dependent CKD (20%; standardized difference=0.12) and those without pre-existing CKD (12%; standardized difference=0.36). Half of dialysis and non-dialysis-dependent CKD patients died within 28 days of ICU admission versus 35% of patients without pre-existing CKD. Compared to patients without pre-existing CKD, dialysis patients had higher risk for 28-day in-hospital death (adjusted HR, 1.41 [95% CI, 1.09-1.81]), while patients with non-dialysis-dependent CKD had an intermediate risk (adjusted HR, 1.25 [95% CI, 1.08-1.44]).
Potential residual confounding.
Findings highlight the high mortality of individuals with underlying kidney disease and severe COVID-19, underscoring the importance of identifying safe and effective COVID-19 therapies in this vulnerable population.
肾脏疾病是导致 2019 年冠状病毒病(COVID-19)病情加重的一个新出现的危险因素。本研究旨在探讨合并和不合并慢性肾脏病(CKD)的危重症 COVID-19 患者的临床病程,并探讨基础肾脏疾病的严重程度与住院结局之间的关系。
回顾性队列研究。
美国 68 家医院的重症监护病房(ICU)收治的 4264 例 COVID-19 危重症患者(143 例存在基础肾衰竭并接受维持性透析的患者;521 例存在基础非透析依赖性 CKD 的患者;3600 例不存在基础 CKD 的患者)。
是否存在基础肾脏疾病。
院内死亡率(主要结局);呼吸衰竭、休克、室性心律失常/心搏骤停、血栓栓塞事件、大出血和急性肝损伤(次要结局)。
采用标准化差值比较患者特征(差值>0.10 提示组间存在有意义差异),并采用多变量调整后的 Fine 和 Gray 生存模型来检验结局相关性。
与其他组相比,接受透析治疗的患者从症状出现到 ICU 入院的时间更短(维持性透析患者为 4[IQR,2-9]天;非透析依赖性 CKD 患者为 7[IQR,3-10]天;无基础 CKD 的患者为 7[IQR,4-10]天)。与非透析依赖性 CKD 患者(20%;标准化差值=0.12)和无基础 CKD 的患者(12%;标准化差值=0.36)相比,更多的透析患者(25%)报告存在精神状态改变。半数透析和非透析依赖性 CKD 患者在 ICU 入院后 28 天内死亡,而无基础 CKD 的患者这一比例为 35%。与无基础 CKD 的患者相比,透析患者的 28 天院内死亡率更高(校正 HR,1.41[95%CI,1.09-1.81]),而非透析依赖性 CKD 患者的死亡率处于中间水平(校正 HR,1.25[95%CI,1.08-1.44])。
存在潜在的混杂因素。
研究结果突显了基础肾脏疾病合并严重 COVID-19 患者的高死亡率,强调了在这一脆弱人群中确定安全有效的 COVID-19 治疗方法的重要性。