Home P D, Jones N P, Pocock S J, Beck-Nielsen H, Gomis R, Hanefeld M, Komajda M, Curtis P
Newcastle Diabetes Centre and Newcastle University, UK.
Diabet Med. 2007 Jun;24(6):626-34. doi: 10.1111/j.1464-5491.2007.02160.x.
To compare glucose control over 18 months between rosiglitazone oral combination therapy and combination metformin and sulphonylurea in people with Type 2 diabetes.
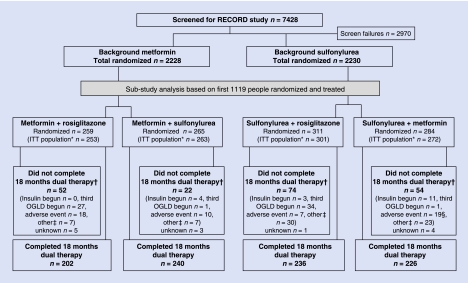
RECORD, a multicentre, parallel-group study of cardiovascular outcomes, enrolled people with an HbA(1c) of 7.1-9.0% on maximum doses of metformin or sulphonylurea. If on metformin they were randomized to add-on rosiglitazone or sulphonylurea (open label) and if on sulphonylurea to rosiglitazone or metformin. HbA(1c) was managed to < or = 7.0% by dose titration. A prospectively defined analysis of glycaemic control on the first 1122 participants is reported here, with a primary outcome assessed against a non-inferiority margin for HbA(1c) of 0.4%.
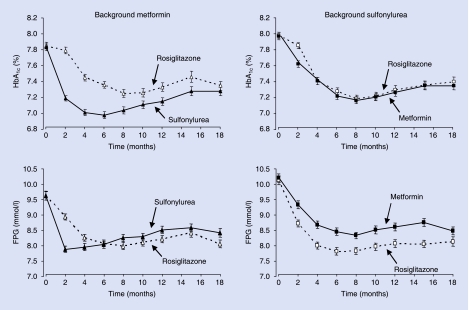
At 18 months, HbA(1c) reduction on background metformin was similar with rosiglitazone and sulphonylurea [difference 0.07 (95% CI -0.09, 0.23)%], as was the change when rosiglitazone or metformin was added to sulphonylurea [0.06 (-0.09, 0.20)%]. At 6 months, the effect on HbA(1c) was greater with add-on sulphonylurea, but was similar whether sulphonylurea was added to rosiglitazone or metformin. Differences in fasting plasma glucose were not statistically significant at 18 months [rosiglitazone vs. sulphonylurea -0.36 (-0.74, 0.02) mmol/l, rosiglitazone vs. metformin -0.34 (-0.73, 0.05) mmol/l]. Increased homeostasis model assessment insulin sensitivity and reduced C-reactive protein were greater with rosiglitazone than metformin or sulphonylurea (all P < or = 0.001). Body weight was significantly increased with rosiglitazone compared with sulphonylurea [difference 1.2 (0.4, 2.0) kg, P = 0.003] and metformin [difference 4.3 (3.6, 5.1) kg, P < 0.001].
In people with diabetes, rosiglitazone in combination with metformin or sulphonylurea was demonstrated to be non-inferior to the standard combination of metformin + sulphonylurea in lowering HbA(1c) over 18 months, and produces greater improvements in C-reactive protein and basal insulin sensitivity but is also associated with greater weight gain.
比较罗格列酮口服联合疗法与二甲双胍和磺脲类药物联合疗法对2型糖尿病患者18个月的血糖控制情况。
RECORD是一项关于心血管结局的多中心、平行组研究,纳入了服用最大剂量二甲双胍或磺脲类药物且糖化血红蛋白(HbA1c)为7.1 - 9.0%的患者。如果患者正在服用二甲双胍,他们被随机分配加用罗格列酮或磺脲类药物(开放标签);如果正在服用磺脲类药物,则被随机分配加用罗格列酮或二甲双胍。通过剂量滴定将HbA1c控制在≤7.0%。本文报告了对前1122名参与者血糖控制的前瞻性定义分析,主要结局根据HbA1c非劣效界值0.4%进行评估。
18个月时,在二甲双胍基础上加用罗格列酮和磺脲类药物后的HbA1c降低情况相似[差值0.07(95%可信区间 -0.09,0.23)%],在磺脲类药物基础上加用罗格列酮或二甲双胍时的变化情况也相似[0.06(-0.09,0.20)%]。6个月时,加用磺脲类药物对HbA1c的影响更大,但无论磺脲类药物是加用在罗格列酮还是二甲双胍上,效果相似。18个月时空腹血糖差异无统计学意义[罗格列酮与磺脲类药物比较为 -0.36(-0.74,0.02)mmol/L,罗格列酮与二甲双胍比较为 -0.34(-0.73,0.05)mmol/L]。与二甲双胍或磺脲类药物相比,罗格列酮使稳态模型评估胰岛素敏感性增加和C反应蛋白降低的幅度更大(所有P≤0.001)。与磺脲类药物相比,罗格列酮使体重显著增加[差值1.2(0.4,2.0)kg,P = 0.003],与二甲双胍相比也使体重显著增加[差值4.3(3.6,5.1)kg,P<0.001]。
对于糖尿病患者,罗格列酮联合二甲双胍或磺脲类药物在降低HbA1c方面被证明在18个月内不劣于二甲双胍 + 磺脲类药物的标准联合疗法,并且在改善C反应蛋白和基础胰岛素敏感性方面效果更显著,但也与更多的体重增加相关。