Minotti J R, Christoph I, Oka R, Weiner M W, Wells L, Massie B M
Cardiology Section, San Francisco Veterans Affairs Medical Center, California 94121.
J Clin Invest. 1991 Dec;88(6):2077-82. doi: 10.1172/JCI115537.
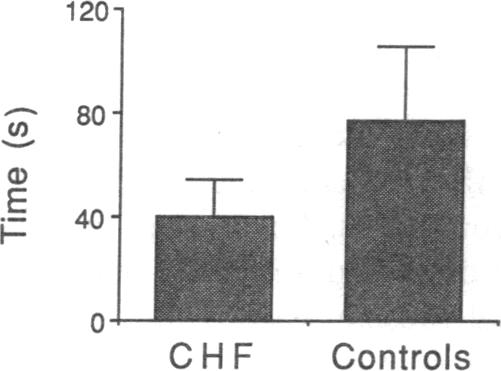
In patients with congestive heart failure (CHF), the poor relationship between systemic exercise performance and cardiac function, together with morphologic and metabolic abnormalities in skeletal muscle, raises the possibility that skeletal muscle function may be impaired and limit systemic exercise performance. We assessed strength and endurance of the knee extensors during static and dynamic exercise in 16 patients with Class I-IV CHF and eight age-matched sedentary controls and related these measurements to systemic exercise performance. To assess skeletal muscle function independent of peripheral blood flow, endurance was repeated under ischemic conditions. Strength was not significantly different in the two groups. Dynamic endurance, quantified as the decline in peak torque during 15 successive isokinetic knee extensions, was significantly reduced in the patients compared to controls during aerobic (peak torque 65 vs. 86% of initial for exercise at 90 deg/s and 60 vs. 85% for exercise at 180 deg/s; P less than 0.002 for both), and during ischemic exercise (56 vs. 76% of initial torque; P less than 0.01). Static endurance, defined as the time required for force during a sustained maximal voluntary contraction to decline to 60% of maximal, was reduced in the patients compared to controls (40 +/- 14 vs. 77 +/- 29 s; P less than 0.02). There were highly significant relationships between systemic exercise performance and skeletal muscle endurance at 90 and 180 deg/s in the patients with CHF (r = 0.90 and 0.66, respectively). These findings indicate that skeletal muscle endurance is impaired in patients with CHF, that this abnormality is in part independent of limb blood flow, and that these changes may be important determinants of systemic exercise performance.
在充血性心力衰竭(CHF)患者中,全身运动能力与心功能之间的不良关系,以及骨骼肌的形态和代谢异常,增加了骨骼肌功能可能受损并限制全身运动能力的可能性。我们评估了16例I-IV级CHF患者和8例年龄匹配的久坐对照者在静态和动态运动期间股四头肌的力量和耐力,并将这些测量结果与全身运动能力相关联。为了独立于外周血流评估骨骼肌功能,在缺血条件下重复进行耐力测试。两组的力量没有显著差异。动态耐力以连续15次等速伸膝过程中峰值扭矩的下降来量化,在有氧运动期间(90度/秒运动时,患者的峰值扭矩为初始值的65%,而对照组为86%;180度/秒运动时,患者为60%,对照组为85%;两者P均小于0.002)以及缺血运动期间(患者为初始扭矩的56%,对照组为76%;P小于0.01),患者的动态耐力明显低于对照组。静态耐力定义为持续最大自主收缩时力量下降到最大值的60%所需的时间,患者的静态耐力低于对照组(40±14秒对77±29秒;P小于0.02)。在CHF患者中,全身运动能力与90度/秒和180度/秒时的骨骼肌耐力之间存在高度显著的相关性(r分别为0.90和0.66)。这些发现表明,CHF患者的骨骼肌耐力受损,这种异常部分独立于肢体血流,并且这些变化可能是全身运动能力的重要决定因素。