Zhang Miao, Moiseenko Vitali, Liu Mitchell
Department of Medical Physics, British Columbia Cancer Agency-Fraser Valley Centre, Surrey, British Columbia, Canada.
J Appl Clin Med Phys. 2006 May 25;7(2):38-49. doi: 10.1120/jacmp.v7i2.2210.
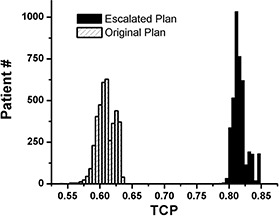
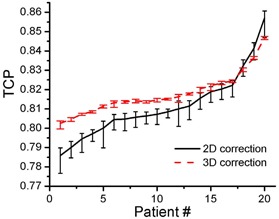
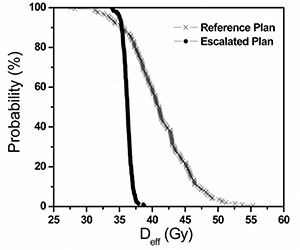
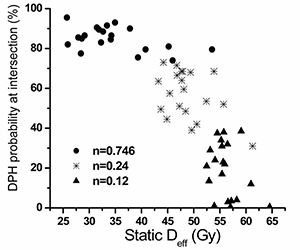
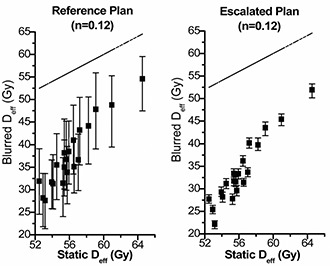
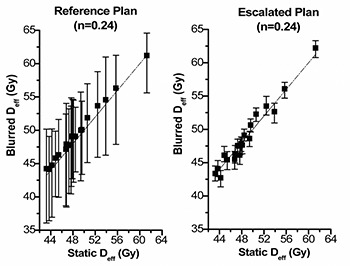
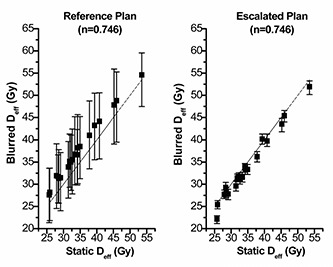
Using internal fiducial markers and electronic portal imaging (EPID) to realign patients has been shown to significantly reduce positioning uncertainties in prostate radiation treatment. This creates the possibility of decreasing the planning target volume (PTV) margin added on the clinical target volume (CTV), which in turn may allow for dose escalation. We compared the outcome of two plans: 70Gy/35fx, 10 mm PTV margin without patient realignment (Reference Plan) vs. 78Gy/39fx, 5 mm PTV margin with patient realignment (Escalated Plan). Four-field-oblique (gantry angles 35 degrees, 90 degrees, 270 degrees, 176 degrees, 325 degrees) beam arrangement was used. Monte Carlo code was used to simulate the daily organ motion. Dose to each organ was calculated. Tumour control probability (TCP) and the effective dose to critical organ (Deff) were calculated using the biologically normalized dose-volume histograms. By comparing the biological factors, we found that the prescription dose can be escalated to 78Gy/39fx with a 5 mm PTV margin when using internal fiducial markers and EPID. Based on the available dose-response data for intermediate risk prostate patients, this will result in a 20% increase of local control and significantly reduced rectal complications provided that less serial dose-volume behaviour of rectum is proven.
使用内部基准标记和电子射野影像装置(EPID)对患者进行重新定位已被证明可显著降低前列腺放射治疗中的定位不确定性。这使得有可能减小在临床靶区(CTV)上增加的计划靶区(PTV)边界,进而可能允许提高剂量。我们比较了两个计划的结果:70Gy/35次分割,无患者重新定位时PTV边界为10mm(参考计划)与78Gy/39次分割,有患者重新定位时PTV边界为5mm(提高剂量计划)。采用四野斜野(机架角度为35度、90度、270度、176度、325度)射束排列。使用蒙特卡罗代码模拟每日器官运动。计算每个器官的剂量。使用生物归一化剂量体积直方图计算肿瘤控制概率(TCP)和关键器官的有效剂量(Deff)。通过比较生物学因素,我们发现当使用内部基准标记和EPID时,处方剂量可提高到78Gy/39次分割,PTV边界为5mm。根据中度风险前列腺患者现有的剂量反应数据,这将使局部控制提高20%,并且如果直肠的串行剂量体积行为得到证实,则可显著降低直肠并发症。