Amin Abdinasir A, Zurovac Dejan, Kangwana Beth B, Greenfield Joanne, Otieno Dorothy N, Akhwale Willis S, Snow Robert W
Malaria Public Health & Epidemiology Group, Centre for Geographic Medicine Research-Coast, Kenya Medical Research Institute/Wellcome Trust Research Programme, Nairobi, Kenya.
Malar J. 2007 May 29;6:72. doi: 10.1186/1475-2875-6-72.
Sulphadoxine/sulphalene-pyrimethamine (SP) was adopted in Kenya as first line therapeutic for uncomplicated malaria in 1998. By the second half of 2003, there was convincing evidence that SP was failing and had to be replaced. Despite several descriptive investigations of policy change and implementation when countries moved from chloroquine to SP, the different constraints of moving to artemisinin-based combination therapy (ACT) in Africa are less well documented.
A narrative description of the process of anti-malarial drug policy change, financing and implementation in Kenya is assembled from discussions with stakeholders, reports, newspaper articles, minutes of meetings and email correspondence between actors in the policy change process. The narrative has been structured to capture the timing of events, the difficulties and hurdles faced and the resolutions reached to the final implementation of a new treatment policy.
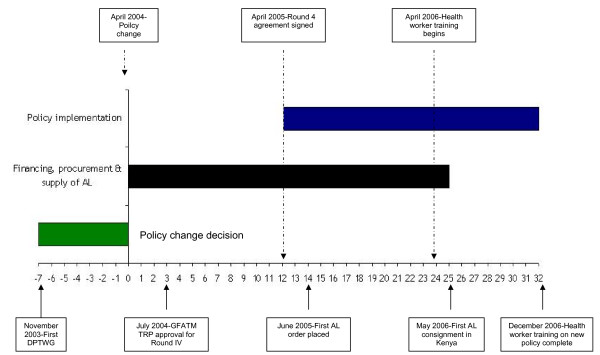
Following a recognition that SP was failing there was a rapid technical appraisal of available data and replacement options resulting in a decision to adopt artemether-lumefantrine (AL) as the recommended first-line therapy in Kenya, announced in April 2004. Funding requirements were approved by the Global Fund to Fight AIDS, Tuberculosis and Malaria (GFATM) and over 60 million US$ were agreed in principle in July 2004 to procure AL and implement the policy change. AL arrived in Kenya in May 2006, distribution to health facilities began in July 2006 coincidental with cascade in-service training in the revised national guidelines. Both training and drug distribution were almost complete by the end of 2006. The article examines why it took over 32 months from announcing a drug policy change to completing early implementation. Reasons included: lack of clarity on sustainable financing of an expensive therapeutic for a common disease, a delay in release of funding, a lack of comparative efficacy data between AL and amodiaquine-based alternatives, a poor dialogue with pharmaceutical companies with a national interest in antimalarial drug supply versus the single sourcing of AL and complex drug ordering, tendering and procurement procedures.
Decisions to abandon failing monotherapy in favour of ACT for the treatment of malaria can be achieved relatively quickly. Future policy changes in Africa should be carefully prepared for a myriad of financial, political and legislative issues that might limit the rapid translation of drug policy change into action.
1998年,磺胺多辛/磺胺林-乙胺嘧啶(SP)在肯尼亚被用作非复杂性疟疾的一线治疗药物。到2003年下半年,有确凿证据表明SP治疗失败,必须予以更换。尽管在各国从氯喹转向SP时,对政策变化和实施情况进行了多项描述性调查,但在非洲转向以青蒿素为基础的联合疗法(ACT)所面临的不同制约因素记录较少。
通过与利益相关者的讨论、报告、报纸文章、会议记录以及政策变化过程中各方之间的电子邮件通信,对肯尼亚抗疟药物政策变化、筹资和实施过程进行了叙述性描述。叙述的结构旨在把握事件的时间安排、面临的困难和障碍以及新治疗政策最终实施所达成的解决方案。
在认识到SP治疗失败后,对现有数据和替代方案进行了快速技术评估,结果决定采用蒿甲醚-本芴醇(AL)作为肯尼亚推荐的一线治疗药物,并于2004年4月宣布。抗击艾滋病、结核病和疟疾全球基金(GFATM)批准了资金需求,2004年7月原则上同意提供6000多万美元用于采购AL并实施政策变更。AL于2006年5月抵达肯尼亚,2006年7月开始向卫生设施分发,同时开展修订后的国家指南的级联在职培训。到2006年底,培训和药物分发几乎全部完成。本文探讨了为何从宣布药物政策变更到完成早期实施耗时超过32个月。原因包括:对一种常见疾病的昂贵治疗药物的可持续筹资缺乏明确性、资金发放延迟、AL与基于阿莫地喹的替代药物之间缺乏比较疗效数据、与对疟疾药物供应具有国家利益的制药公司缺乏良好对话、AL的单一采购以及复杂的药物订购、招标和采购程序。
决定放弃失败的单一疗法而采用ACT治疗疟疾可以相对迅速地实现。非洲未来的政策变化应针对可能限制药物政策变化迅速转化为行动的众多财务、政治和立法问题进行精心准备。