Singhal Vinay, Bansal Anju, Bhatnagar Dinesh, Saxena Sunita
Department of Surgery, Vardhman Mahavir Medical College, Safdarjang Hospital, New, Delhi, India.
World J Surg Oncol. 2007 May 13;5:52. doi: 10.1186/1477-7819-5-52.
Colostomy site carcinomas are rare with only eight cases reported in the world literature. Various etiological factors like adenoma-cancer sequence, bile acids, recurrent and persistent physical damage at the colostomy site by faecal matter due to associated stomal stenosis have been considered responsible. Two such cases are being reported and in both cases there was no evidence of any local recurrence in the pelvis or liver and distant metastasis. Both patients had received adjuvant chemotherapy following surgery.
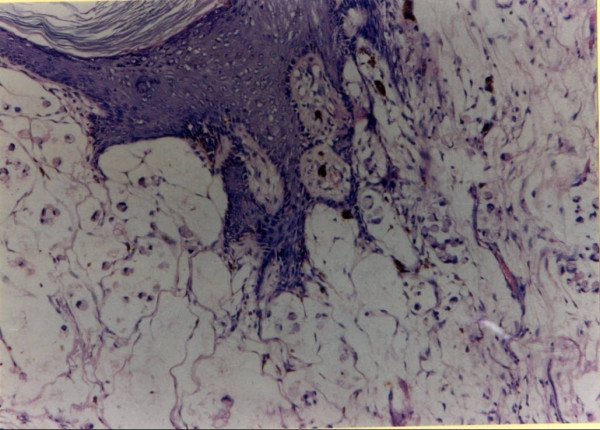
First case was a 30-year-old male that had reported with large bowel obstruction due to an obstructing ulcero-proliferative growth (poorly differentiated adenocarcinoma) at the colostomy site after abdomino-perineal resection, performed for low rectal cancer six years previously. Wide local excision with microscopically free margins was performed with a satisfactory outcome. Four years later he presented with massive malignant ascites, cachexia and multiple liver metastasis and succumbed to his disease. Second case was a 47-year-old male that presented with acute large bowel obstruction due to an annular growth (well differentiated adenocarcinoma) in the upper rectum. He was managed by Hartmann's operation and the sigmoid colostomy was closed six months later. Five years following closure of colostomy, he presented with two parietal masses at the previous colostomy site scar, which, on fine needle aspiration cytology were found to be well-differentiated adenocarcinomas of colorectal type. Surgery in the form of wide local resection with free margins was performed. He presented again after five years with recurrence along the previous surgery scar and an incisional hernia and was managed by wide local excision along with hernioplasty. Follow-up of nine years following first surgery is satisfactory.
Colostomy site/scar recurrence of rectal carcinoma is rare and could be due to various etiological factors, although the exact causative mechanism is not known. Surgery with microscopically free margins is recommended in the absence of metastatic disease. Stenosis of the stoma is considered as one of the most important contributory factors and should be followed carefully.
结肠造口部位癌很罕见,世界文献中仅报道了8例。多种病因因素,如腺瘤-癌序列、胆汁酸、由于相关造口狭窄导致粪便对结肠造口部位反复和持续的物理损伤等,都被认为与此有关。现报告两例此类病例,两例均无盆腔或肝脏局部复发及远处转移的证据。两名患者术后均接受了辅助化疗。
第一例是一名30岁男性,因六年前因低位直肠癌行腹会阴切除术后,结肠造口部位出现阻塞性溃疡增生性肿物(低分化腺癌)导致大肠梗阻前来就诊。进行了切缘显微镜下无癌残留的广泛局部切除,效果满意。四年后,他出现大量恶性腹水、恶病质和多发肝转移,最终因病死亡。第二例是一名47岁男性,因上段直肠环形肿物(高分化腺癌)导致急性大肠梗阻前来就诊。他接受了哈特曼手术治疗,六个月后关闭了乙状结肠造口。结肠造口关闭五年后,他在原结肠造口部位瘢痕处出现两个腹壁肿物,细针穿刺细胞学检查发现为结直肠型高分化腺癌。进行了切缘无癌残留的广泛局部切除手术。五年后他再次出现,原手术瘢痕处复发并伴有切口疝,接受了广泛局部切除及疝修补术。首次手术后九年的随访情况良好。
直肠癌结肠造口部位/瘢痕复发罕见,可能由多种病因因素导致,尽管确切的致病机制尚不清楚。在无转移性疾病的情况下,建议进行切缘显微镜下无癌残留的手术。造口狭窄被认为是最重要的促成因素之一,应密切随访。