Aarts F, Hendriks T, Boerman O C, Koppe M J, Oyen W J G, Bleichrodt R P
Department of Surgery, Radboud University Nijmegen Medical Centre, PO Box 9101, 6500, HB, Nijmegen, The Netherlands.
Ann Surg Oncol. 2007 Nov;14(11):3274-82. doi: 10.1245/s10434-007-9509-2. Epub 2007 Jul 25.
Cytoreductive surgery (CS) followed by heated intraperitoneal chemotherapy (HIPEC) is considered the standard of care for the treatment of patients with peritoneal carcinomatosis (PC) of colorectal cancer (CRC). These surgical procedures result in a median survival of 2 years at the cost of considerable morbidity and mortality. In preclinical studies, radioimmunotherapy (RIT) improved survival after CS in a model of induced PC of colonic origin. In the present studies we aimed to compare the efficacy and toxicity of CS followed by adjuvant RIT in experimental PC to the standard of care, HIPEC.
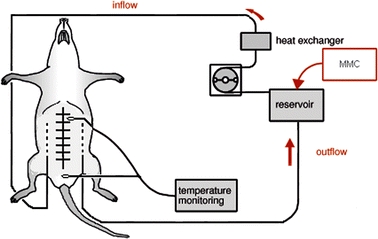
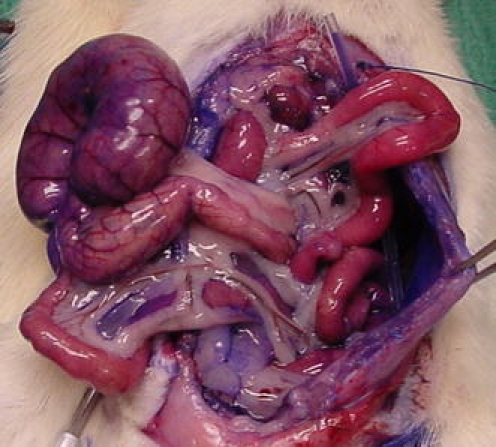
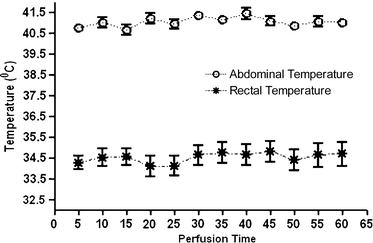
PC was induced by intraperitoneal inoculation of CC-531 colon carcinoma cells in three groups of Wag/Rij rats. Treatment comprised CS only, CS + RIT or CS + HIPEC, immediately after surgery. RIT consisted of intraperitoneal administration of 74 MBq Lutetium-177 labeled MG1. HIPEC was performed by a closed abdomen perfusion technique using mitomycin C (16 mg/L during 60 minutes). The primary endpoint was survival.
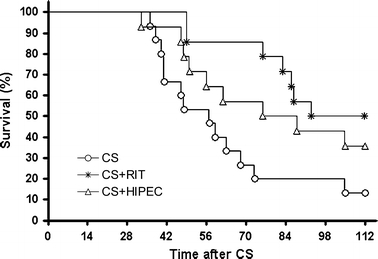
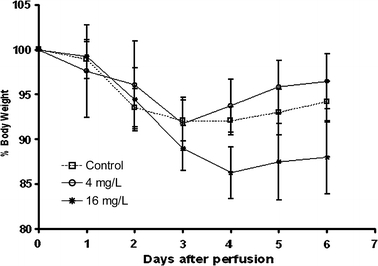
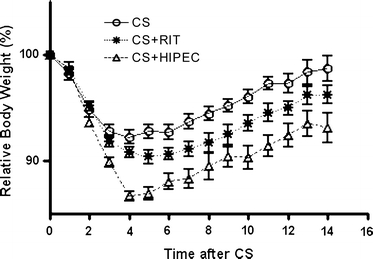
CS only or combined with RIT was well tolerated. Rats receiving CS + HIPEC were lethargic, suffered from diarrhea, and lost significantly more weight in the first postoperative week. Median survival of rats treated with CS + RIT was significantly longer than after CS alone (97 and 57 days, respectively, P < .004), whereas survival after CS + HIPEC or CS alone were not significantly different (76 and 57 days, respectively, P = .17).
Survival after CS was significantly improved by RIT with Lutetium-177-MG1 in rats with PC of colorectal origin. Adjuvant HIPEC did not improve survival and was more toxic than adjuvant RIT.
细胞减灭术(CS)联合热腹腔内化疗(HIPEC)被认为是治疗结直肠癌(CRC)腹膜癌转移(PC)患者的标准治疗方案。这些手术操作使患者的中位生存期达到2年,但代价是较高的发病率和死亡率。在临床前研究中,放射免疫疗法(RIT)在结肠源性PC诱导模型中改善了CS后的生存率。在本研究中,我们旨在比较CS联合辅助RIT与标准治疗方案HIPEC在实验性PC中的疗效和毒性。
通过向三组Wag/Rij大鼠腹腔内接种CC-531结肠癌细胞诱导PC。治疗方案包括术后立即仅行CS、CS + RIT或CS + HIPEC。RIT包括腹腔内注射74 MBq镥-177标记的MG1。HIPEC采用闭腹灌注技术,使用丝裂霉素C(60分钟内16 mg/L)。主要终点是生存期。
单纯CS或联合RIT耐受性良好。接受CS + HIPEC的大鼠无精打采,出现腹泻,且在术后第一周体重明显减轻更多。接受CS + RIT治疗的大鼠中位生存期明显长于单纯CS组(分别为97天和57天,P <.004),而CS + HIPEC组或单纯CS组的生存期无显著差异(分别为76天和57天,P =.17)。
在结直肠源性PC大鼠中,镥-177-MG1的RIT显著提高了CS后的生存率。辅助HIPEC未改善生存率,且比辅助RIT毒性更大。