Bernhard J, Zahrieh D, Zhang J J, Martinelli G, Basser R, Hürny C, Forbes J F, Aebi S, Yeo W, Thürlimann B, Green M D, Colleoni M, Gelber R D, Castiglione-Gertsch M, Price K N, Goldhirsch A, Coates A S
IBCSG Coordinating Center, Effingerstrasse 40, Bern 3008, Switzerland.
Br J Cancer. 2008 Jan 15;98(1):25-33. doi: 10.1038/sj.bjc.6604092. Epub 2007 Nov 27.
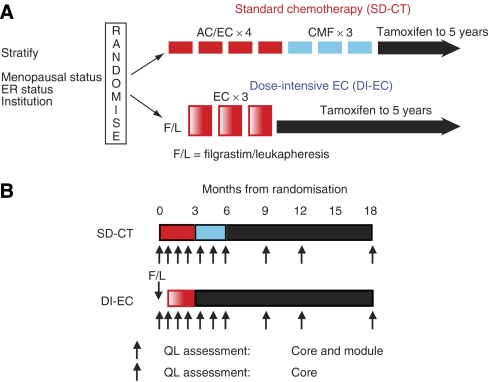
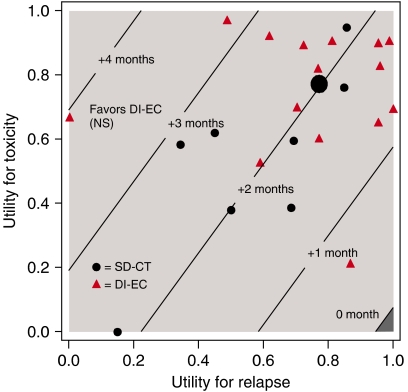
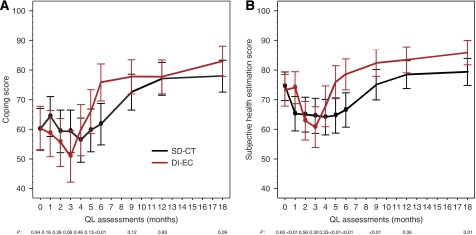
Quality of life (QL) is an important consideration when comparing adjuvant therapies for early breast cancer, especially if they differ substantially in toxicity. We evaluated QL and Q-TWiST among patients randomised to adjuvant dose-intensive epirubicin and cyclophosphamide administered with filgrastim and progenitor cell support (DI-EC) or standard-dose anthracycline-based chemotherapy (SD-CT). We estimated the duration of chemotherapy toxicity (TOX), time without disease symptoms and toxicity (TWiST), and time following relapse (REL). Patients scored QL indicators. Mean durations for the three transition times were weighted with patient reported utilities to obtain mean Q-TWiST. Patients receiving DI-EC reported worse QL during TOX, especially treatment burden (month 3: P<0.01), but a faster recovery 3 months following chemotherapy than patients receiving SD-CT, for example, less coping effort (P<0.01). Average Q-TWiST was 1.8 months longer for patients receiving DI-EC (95% CI, -2.5 to 6.1). Q-TWiST favoured DI-EC for most values of utilities attached to TOX and REL. Despite greater initial toxicity, quality-adjusted survival was similar or better with dose-intensive treatment as compared to standard treatment. Thus, QL considerations should not be prohibitive if future intensive therapies show superior efficacy.
在比较早期乳腺癌的辅助治疗方案时,生活质量(QL)是一个重要的考量因素,尤其是当这些治疗方案在毒性方面存在显著差异时。我们评估了随机接受辅助性剂量密集型表柔比星和环磷酰胺联合非格司亭及祖细胞支持治疗(DI-EC)或标准剂量蒽环类化疗(SD-CT)的患者的生活质量和质量调整无病生存期(Q-TWiST)。我们估算了化疗毒性持续时间(TOX)、无疾病症状和毒性时间(TWiST)以及复发后时间(REL)。患者对生活质量指标进行评分。通过患者报告的效用值对三个过渡时间的平均持续时间进行加权,以获得平均Q-TWiST。接受DI-EC治疗的患者在化疗毒性期报告的生活质量较差,尤其是治疗负担(第3个月:P<0.01),但化疗后3个月的恢复速度比接受SD-CT治疗的患者更快,例如应对努力更少(P<0.01)。接受DI-EC治疗的患者的平均Q-TWiST长1.8个月(95%可信区间,-2.5至6.1)。对于大多数赋予TOX和REL的效用值,Q-TWiST更倾向于DI-EC。尽管初始毒性更大,但与标准治疗相比,剂量密集型治疗的质量调整生存期相似或更好。因此,如果未来的强化治疗显示出卓越的疗效,生活质量方面的考量不应成为阻碍。